i bc27f85be50b71b1 (182 page)
Read i bc27f85be50b71b1 Online
Authors: Unknown

Osmosis is the movemenr of fluid from an area of lesser solute concentration to an area of greater solute concentration. Ultrafiltration, the removal of water and fluid, is accomplished by creating pressure
gradients between the arterial blood and the dialyzer membrane or
compartment. IS
Another method to manage patients with ARF who are critically ill
is continuous renal replacement therapy, either through continuous
arteriovenous hemofiltrarion (CAVH) or continuous venovenous
hemofiltration (CYVH).lo.ls
Peritoneal Dialysis
Peritoneal dialysis (PO) involves using the peritoneal cavity as a
semipermeable membrane to exchange soluble substances and
water between the dialysate fluid and the blood vessels in the
abdominal cavity.8,lo.ls

588
ACt.JTE CARE HANDBOOK FOR PHYSICAl THFRAPISTS
Dialysate fluid is instilled into the perironeal cavity through an
indwelling catheter that is either placed surgically or nonsurgically.
Surgical placement is preferable, as direct visualization during the
procedure facilitates berrer placement. After the dialysate is instilled
into the peritoneum, there is an equilibration period when water and
solutes pass through the semipermeable membrane. Once equilibration is finished, then the perironeal cavity is drained of the excess fluid and solutes that the failing kidneys cannot remove. Instillation, equilibration, and drainage constitute one exchange. 15
The process of perironeal dialysis can range from 45 minutes ro 9
hours, depending on the method of PO, and patients can have anywhere from four to 24 exchanges per day."
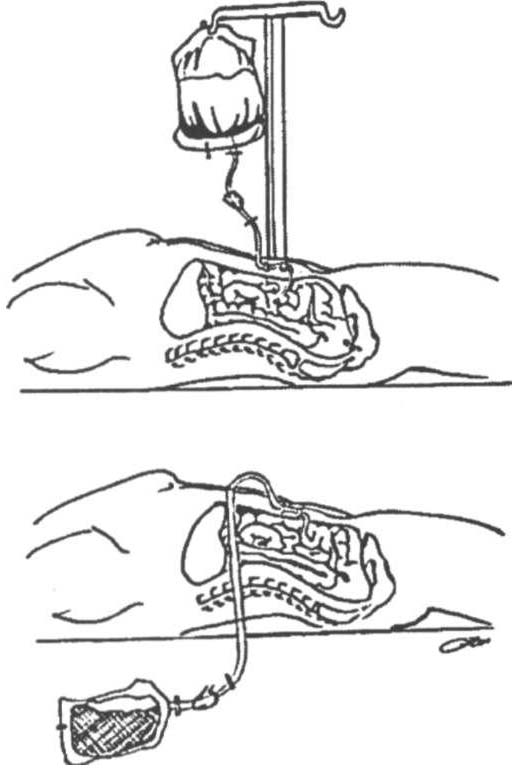
There are two types of PO, auromated PO and continuous ambulatory PD. Automated PD uses an automatic cycling device to control the instillation, equilibration, and drainage phase . ContiullOus
ambulatory PO involves manually exchanging dialysate fluids four
times a day and is schematically represented in Figure 9-3.'5
The following are indications for perironeal dialysis··s:
•
Need for less rapid management of fluid and electrolyte imbalances
• Staff and equipment for hemodialysis unavailable
•
Inadequate vascular access for hemodialysis
•
Shock
• Status post cardiac surgery (e.g., coronary arrery bypass grafting)
• Severe cardiovascular disease
•
Patient refusal of blood transfusions
The following are conrraindications for peritoneal dialysis:
• Peritonitis
• Abdominal adhesions
• Hernias
• Concurrent pulmonary complications, such as atelectasis or
pneumonia
•
Recent abdominal surgery

GENITOURINARY SYSTEM
589
A
B
Figure 9-3. Schematic illustratio" of coutinuous ambulatory peritoueal dialysis. A. l"stillatioN of dialysate fluid. B. Drainage of excess fluid and solutes.
(Artwork by Peter IV".)
Intermittent Hemodialysis
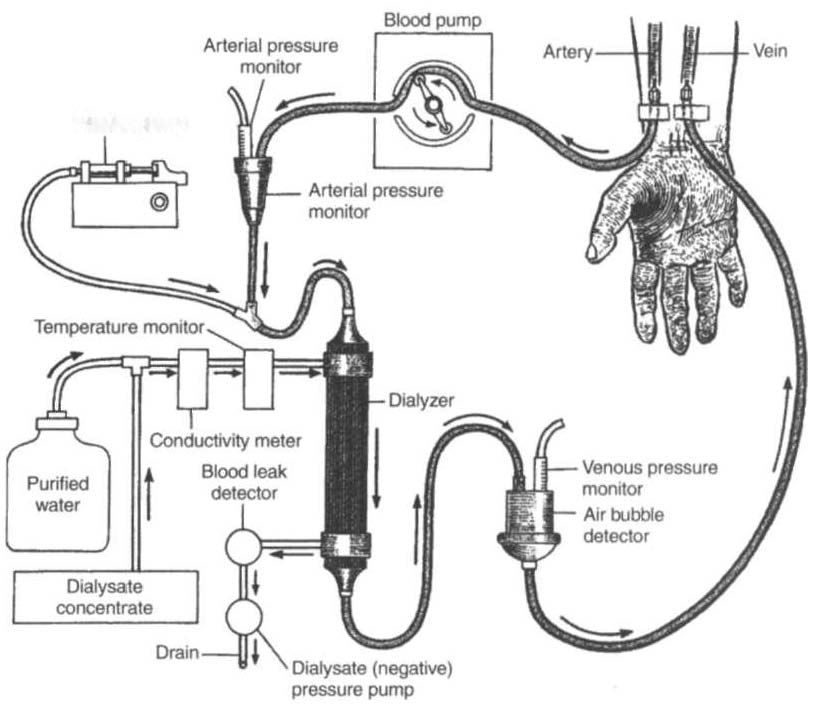
Kidney functions that are controlled by intermittent hemodialysis
include ( I) fluid volume, (2) electrolyte balance, (3) acid-base balance,
and (4) filtration of nitrogenous waStes. The patient's arterial blood is
mechanically circulated through semipermeable tubing that is surrounded by a dialysate solution in the dialyzer (artificial kidney). The dialysate fluid contains electrolytes similar to those in normal blood
plasma ro permit diffusion of electrolytes into Ot out of the patient'S
blood.6•s As the patient'S arterial blood is being filtered through the
dialyzer, "clean" blood is returned to the patient'S venous circulation.
Figure 9-4 illustrates this process.



590
ACUTE CARE HANDBOOK FOR I'HYSICAL THERAPI�TS
Infusion pump
Figure 9-4. Schematic represe"tation of hemodialysis. (With permission from
1M Thompson, GK McFarland, IE Hirsch, et al. (eds(. Mosby's Clinical Nllrsing (]rd ed(. St. LOllis: Mosby, 199];9]8.)
Vascular access is attained either through cannula insertion (usually for temporary dialysis) or through an internal arteriovenous fistula (for chronic dialysis use), which is surgically created in the forearm. The arteriovenous fistula is created by performing a side-toside, side-to-end, or end-to-end anastomosis between the radial or ulnar artery and the cephalic vein. If a native fistula cannot be created, then a synthetic graft is surgically anastomosed between the arterial and venous circulation.6.8.ls Figure 9-5 illu trates these various types of vascular access.
Patients who require chronic intermittent hemodialysis usually
have it administered three to four times per week, with each exchange
lasting approximately 3-4 hours. The overall intent of this process is
to extract up to 2 days' worth of excess fluid and solutes from the
patient'S blood.IO
