i bc27f85be50b71b1 (34 page)
Read i bc27f85be50b71b1 Online
Authors: Unknown

Table I·A.4. Electroc3rdlographic {EeGl Characteristics 3nd Causes of Arnovenrricul3r Blocks
N3me
ECG ChJracrcristics
Common Causes
PT Considerations
brst-degree AV block
Regular rhythm, rate nor·
Elderly wirh heart disease,
If chronic, need ro be more cmmous
mal 60- 100, prolonged
acute myocarditis, acute �1I
of underlying he3rt disease; if new
PR Interval >0.2 (con·
onset, mOOltOr c1osel)· for pro·
stant).
gression to higher level block.
Second-degree AV block
Irregular rhythm, arrial rare
Acute infection, acme �tI
Symproms are uncommon, as
type I (Wenkebach,
> ventricular rate, usu311y
above.
Mobltz I)
both 60-100; PR Interval
lengthens until P W3ve
appears without 3 QRS
complex.
Second-degree AV block
Irregular rhythm, aerial rate
Anterosepral MI
CHF IS commonj can have dizzl·
type II (Mobitz II)
> ventricular nne, PR
ness, fainting, complete uneon·
('
>-
interval may be normal or
sciousnessj may need pacing
'"
prolonged bur is consr3nr
;;
and PT treatmem; should he
�
for each conducted QRS.
held for medical management.
�
Third-degree AV block
Regular rhythm, arrial rare >
Ameroseprai MI, drug imoxi·
Severe CHFj patient will need med·
§
(complete heart
ventricular rarc.
c3rion, infections, electro·
ical management; a pacer (rem·
;:
block)
lyre imbal3nces, coronary
porary or permanent depending
>
�
artery disease, degenerative
on reversihiliry of eriolob'Y) is
�
sclerotic process of AV can·
almosr always necessary.
"
x
duction system
AV = amoventricubr; ClIF = congestive heart failure; MI = myocardial infarction.
Sources: Data from B Aehlen. ACLS Quick Review Study Guide. St. Louis: Mosby, 1 994; and EK Chung. Manual of Cardiac Arrhythmias. 80s·
....
'D
tOn: Bunerwonh-Heinemann, 1 986.

Appendix 1 -B

82 AClfrE CARE HANDBOOK FOR PHYSICAL THERAPISTS
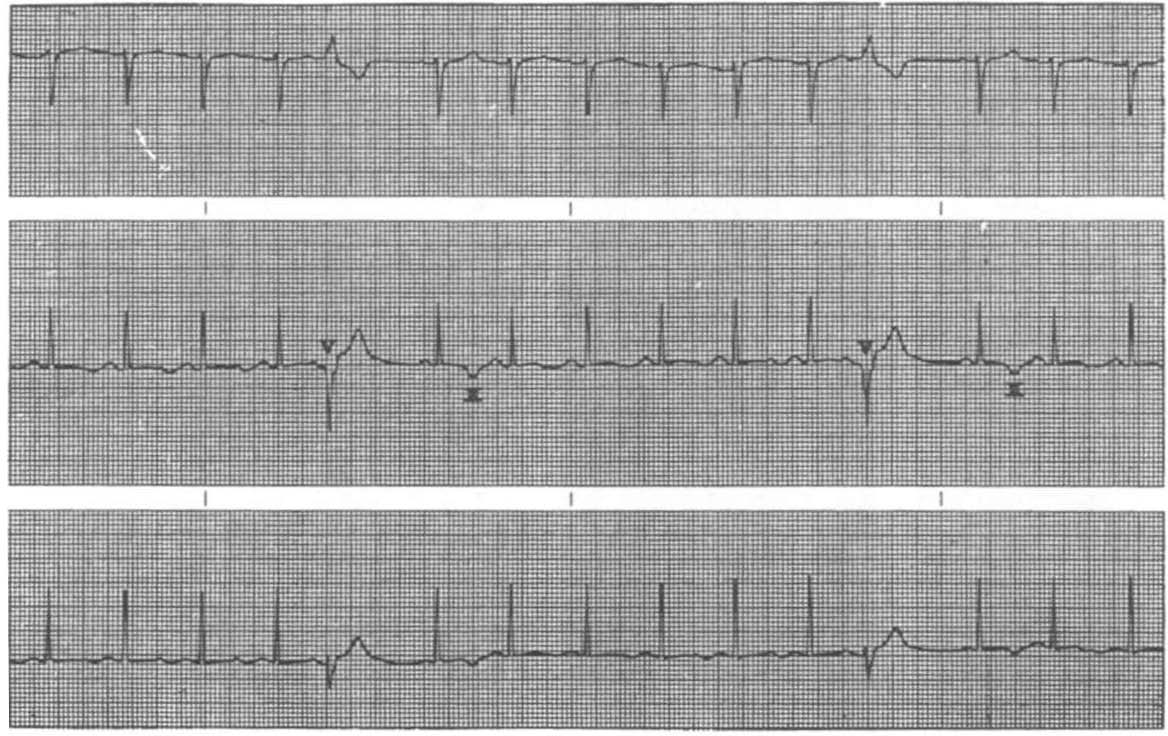
Figure 1-8.1. Paroxysmal supraventricular tachycardia. Note development
from 110rmal sinus rhythm. (\Vith permission from M \'(/alsh, A Crumbie, S
Reveley. Nurse Practitioners: Clinical Skills and Professional lssucs. Boston:
Butterworth-HeiNematm, J 993;96.)
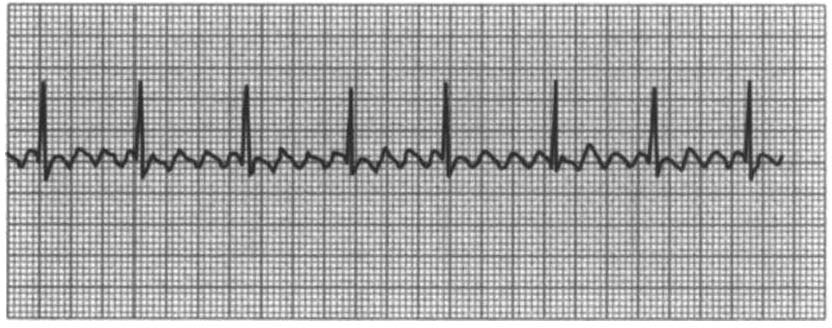
Figure 1-8.2. Atrial {lutter. Note regular rhythm (P waves) but vemriwfar
rhythm depends on CONduction pattern. (\Vith permission fr011l M \Valsh, A
Cmmbie, S RevelC),. Nurse PractitioNers: Clinical Skills and Professional
Issues. Boston: Butterworth-Heinemann, 1 993;95.}

CARDIAC SYSTEM I\PPENDIX ] -B
83
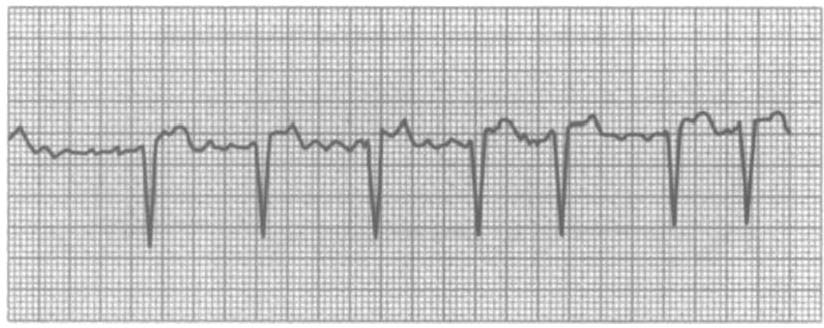
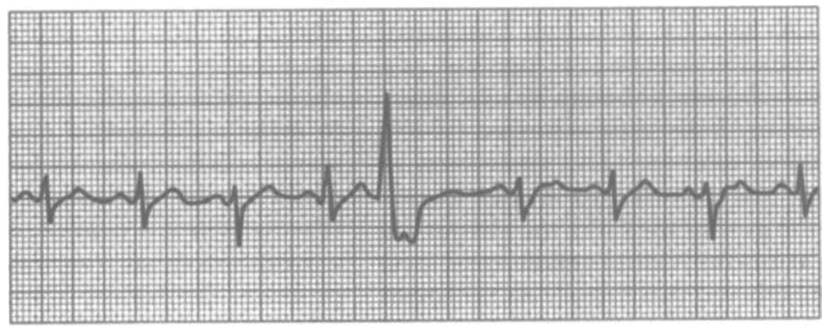
Figure I-B.3. Atrial fibrillation. Note the irregular rhythm alld absence of
normal P waves. (With permission from M Wafsh, A Crumbie, S Reveley.
Nurse Practitioners: Clinical Skills and Pro(essional Issues. Boston: Butterworth-Heinemann, 1 993;95.)
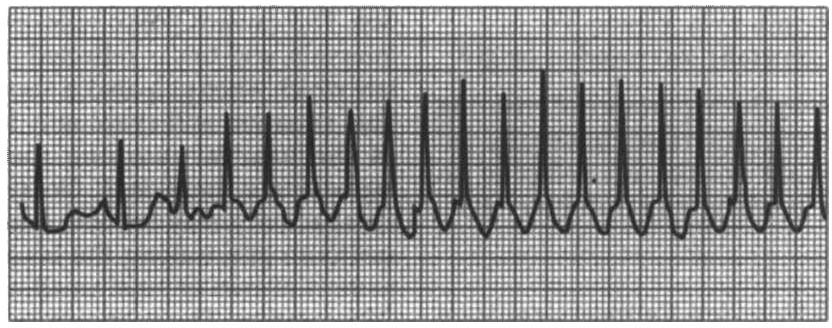
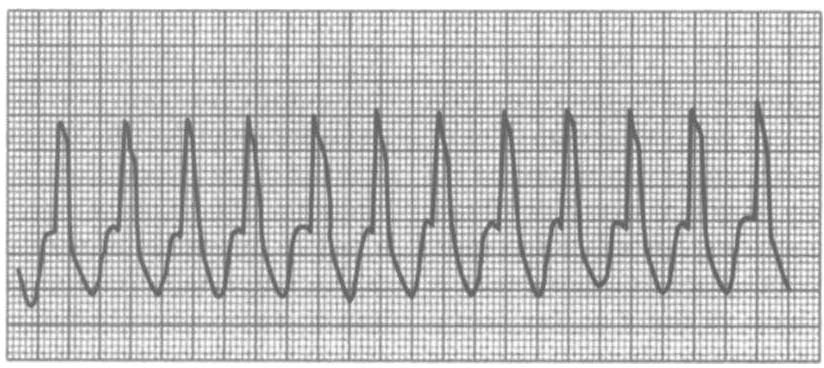
Figure 1-8.4. Ventricular tachycardia. Rate 100-170 beats per minute. No P
waves, broad electrocardiographic wave complexes. (Reprillted with pemlission (rom M Walsh, A Crumbie, S Reveley. Nurse Practitioners: Clinical Skills and 1)ro(essiollal ls5ues. BOSIOI1: Butterworth-Heinemann, 1 993;98.)

84
AClITE CARE HANDBOOK fOR I'HYSICAL THERAI'IS1S
p
p
p
Figure I-B.S. Ventricular ectopy with refractory period afterward. (\Vith permissioN from M \Valsh, A Crumbie, S Reveley. Nurse Praclltioners: Clinical Skills and Professional Issues. Boston: Butterworth-Hememallll, 1 993;97.)