Oxford Handbook of Midwifery (58 page)
Read Oxford Handbook of Midwifery Online
Authors: Janet Medforth,Sue Battersby,Maggie Evans,Beverley Marsh,Angela Walker

- The uterus should return to feeling soft between contractions.
- Contractions may last from 30s up to 90s. The midwife notes the time of the start of the contraction and how long it lasts.
- Uterine contractions are not felt by the woman at the beginning and the end. However the midwife can detect the start of the contraction by palpation before the woman. This may well be useful for using pain relief such as inhalational analgesia or for encouraging coping mechanisms in labour such as breathing and relaxation techniques.
Amniotic
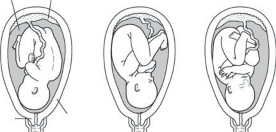
fluid Placenta
Cervix
Uterus(a) Left occipito-anterior (b) Right occipito-lateral (c) Right occipito-posterior
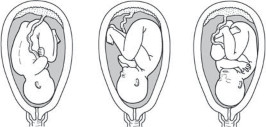

- Right occipito-anterior (e) Left occipito-lateral (f) Left occipito-posterior
Fig. 11.1
Cephalic presentations prior to labour.Reproduced from
Acupuncture in Pregnancy and Childbirth
. Zita West (2001) Copyright © Elsevier Limited 2001, reprinted by permission of the publisher.CHAPTER 11
Normal labour: first stage232
Vaginal examination
In normal labour, vaginal examination is performed at the discretion of the midwife, dependent on the individual needs of the woman, consent, and her progress through labour. Sensitivity should be employed at all times, as many women find vaginal examinations uncomfortable and traumatic. Where possible, examinations should be kept to a minimum (only when clinically indicated) and ideally should be performed by the same person.
Indications
Vaginal examination may be undertaken to:
- Confirm the establishment of labour
- Provide a baseline for subsequent progress
- Assess progress in labour and detect abnormal indices
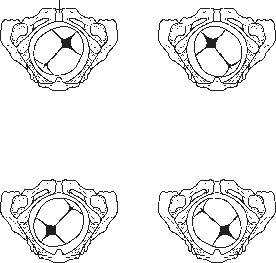
- Assess the presenting part/position if in doubt (Fig. 11.2)
- Confirm the establishment of labour
Symphysis pubis
Occipito-posterior position
Right
Left
Right
Left
Sacrum
right occipito-posterior
Sacrum
left occipito-posterior
Symphysis pubis
Occipito-anterior position

Right
Left
Right
Left
Sacrum
left occipito-anterior
Sacrum
right occipito-anterior
Fig. 11.2
Occipito-anterior and occipito-posterior positions.Reproduced from
Acupuncture in Pregnancy and Childbirth
. Zita West (2001) Copyright © Elsevier Limited 2001, reprinted by permission of the publisher.VAGINAL EXAMINATION
233
- Right occipito-anterior (e) Left occipito-lateral (f) Left occipito-posterior
- Confirm progress to the second stage of labour
- Determine the position and station of the presenting part
- Determine the cause of delay/lack of progress in the second stage
- Rupture membranes if indicated
- Apply a fetal electrode
- Exclude cord prolapse following rupture of the membranes when ill- fitting or non-engagement of the presenting part or polyhydramnios is encountered.
Method
Discussion with the woman is essential before examination, to explain the procedure, reassure, and gain consent.
- Encourage the woman to empty her bladder.
- Assist in making her comfortable.
- Carry out an abdominal examination and auscultation of the fetal heart prior to examination.
- Clean the surrounding labial area/apply gloves (dependent on local policy).
- Assess the external genitalia (lesions, scars, varicose veins, discharge).
- Assess the cervix: consistency, position, effacement and dilatation.
- Assess the membranes: absent or intact, observation of liquor.
- Auscultate the fetal heart after the procedure.

- Explain your findings to the woman.
CHAPTER 11
Normal labour: first stage234
The partogram
The partogram is a graphical overview of the physical elements and events that take place in an individual woman’s labour. This has proved to be an invaluable, at a glance, visual aid and reference for midwives during their care of women in labour. It is especially useful when handing over the woman’s care to a colleague, as it provides an instant summary of the woman’s progress to date. The partogram is usually commenced when the woman is in established labour. Details recorded on the partogram are:
- Hospital number, name of woman, age, parity, date of birth, and expected date of confinement
- The fetal heart rate, plotted at regular intervals (see b Electronic fetal monitoring, p. 238, for NICE guidelines on frequency of auscultation of the fetal heart rate)
- Observation of the liquor, and what time the membranes ruptured
- Cervical dilatation and descent of the presenting part, plotted diagrammatically
- Oxytocic agents if used during labour
- Uterine activity: the length and strength of the contractions per 10min
- Drugs, inhalational analgesia, and non-pharmacological interventions used
- Urinalysis
- Blood pressure and pulse.
Legally the partogram provides a complete and comprehensive record of care and should include the following information:
- Time of birth, gender of baby, and weight
- Any abnormalities noted at birth
- Mode of birth
- Apgar score and any resuscitation/intervention/drugs given to the baby
- Length of the first, second, and third stages of labour
- Blood loss
- Perineal repair or status of perineum
- Whether meconium or urine passed during or post birth
- Feeding intention and summary of feeding/skin to skin contact.
Originally, it was noted that use of the partogram would easily recognize
 cases of prolonged labour, so that appropriate action/intervention could be taken. However, this also tends to create a structured and rigid approach
cases of prolonged labour, so that appropriate action/intervention could be taken. However, this also tends to create a structured and rigid approachto care, which some midwives find restrictive, while not addressing the woman’s individual needs.
- Most research on the first stage of labour is based on a medical model of care, where interventions are commonplace, and may not reflect normal labour and physiology.
- The length of labour may well be much longer than originally anticipated, particularly in primigravid women.
THE PARTOGRAM
235
- Hospital number, name of woman, age, parity, date of birth, and expected date of confinement
Other books
The Beam: Season Two by Sean Platt, Johnny B. Truant
new poems by Tadeusz Rozewicz
Stacey's Emergency by Ann M. Martin
Live Long, Die Short by Roger Landry
Dancing Barefoot: The Patti Smith Story by Dave Thompson
A Perfect Blood by Kim Harrison
Ivy and Bean Bound to Be Bad by Annie Barrows
Sweet in Love by Lee, Nadia
The Last Wolf: A Highplains Shifter Erotic Romance (Wolf Fire Book 1) by Alice Longstaff
Jump Shot by Tiki Barber, Ronde Barber, Paul Mantell