Pediatric Examination and Board Review (62 page)
Read Pediatric Examination and Board Review Online
Authors: Robert Daum,Jason Canel

17.
The age at which a child goes into puberty dependents most on which of the following?
(A) chronological age
(B) height age
(C) weight age
(D) bone age
(E) B and C
18.
Which of the following is not a goal of therapy for lack of sexual development?
(A) age-appropriate secondary sex characteristics
(B) advancement of bone maturation
(C) growth spurt
(D) relieve concerns of immature appearance
(E) B and C
ANSWERS
1.
(B)
Constitutional delay of puberty. This represents the extreme of normal physiologic variation in timing of onset of puberty. Typically the patient is shorter than the mean with a delay in bone maturation (which is usually equal to the height age). They have a normal growth velocity. There is usually a family history of delayed puberty and late growth spurt. Patients will eventually go into puberty and progress through puberty normally. Treatment usually consists of reassurance. Boys can be treated with a short course of low-dose testosterone to give them pubic hair and a slight growth spurt if there is significant psychological distress about their lack of puberty. They need to be monitored closely on treatment to avoid significant advancement of their bone maturation, which could limit their growth potential because of premature epiphyseal closure.
2.
(A)
Kallmann syndrome. In Kallmann syndrome, hyposmia or anosmia is associated with gonadotropin deficiency. It is caused by improper migration of the gonadotropin-releasing hormone (GnRH) neurons and olfactory bulb across the cribriform plate. It is frequently inherited as an X-linked recessive trait but occasionally can be caused by autosomal dominant or recessive inheritance with variable penetrance. There can be significant heterogeneity within the same family with this condition. Associated anomalies may include renal agenesis, midline facial defects, cryptorchidism, microphallus, sensorineural deafness, and visual abnormalities.
3.
(E)
All of the above. Onset of puberty typically depends more on the bone age than the chronological age. A boy with a bone age of 10 would not be expected to be in puberty; thus his gonadotropin levels would be in the prepubertal range in all conditions listed. Once the bone age advances to a pubertal age, gonadotropin levels in boys with hypergonadotropic hypogonadism will become elevated.
4.
(A)
Constitutional delay of puberty. Because puberty corresponds more closely with bone age than with chronological age, a girl with a bone age of 13 years should be in puberty, and lack of puberty at this bone age would suggest hypogonadism. The correlation between bone age and pubertal onset is less clear in obese children because overnutrition often causes an advancement in bone age.
5.
(E)
None of the above. Gonadarche (maturation of the hypothalamic-pituitary gonadal axis) and adrenarche (maturation of the adrenal gland) are two separate processes. Therefore, adrenarche leading to the development of pubic hair can occur without gonadarche.
6.
(E)
All of the above. Nutritional disorders, intense exercise, and occult chronic illness can all affect the hypothalamic GnRH pulse generator and cause delayed puberty. In addition, constitutional delay of growth and puberty tends to run in families.
7.
(C)
Constitutional delay of puberty. Constitutional delay in puberty is the most common cause of delayed puberty in boys. Children with panhypopituitarism causing delayed puberty usually come to attention because of other hormonal deficiencies.
8.
(B)
A radiograph of the left hand and wrist. The several accepted techniques of assessing bone maturation include the Tanner-Whitehouse method and the method of Greulich and Pyle. Both methods focus on the left hand and wrist.
9.
(C)
A 14-year-old. Delayed puberty is defined as the absence of signs of puberty in a child at a chronological age greater than 2 standard deviations above the mean of pubertal development for a given population. In boys, this age is 14 years. This is also the age at which most boys will be starting high school where communal showering is common; thus their concerns regarding lack of puberty increase.
10.
(C)
A 13-year-old
11.
(E)
Sleep-associated rise of LH secretion. The first biochemical sign of puberty is a sleep-associated rise in LH secretion. Puberty begins with pulsatile GnRH secretion, which is followed by pulsatile gonadotropin secretion, which is eventually followed by maturation of the gonads with a gradual increase in sex hormones. The pulsatile GnRH and gonadotropin secretion begins at night and eventually extends throughout the day in later puberty.
12.
(A)
Early morning gonadotropin levels. In very early puberty, levels of gonadotropins and sex steroids are first detectable at night. Thus the best time to check outpatient laboratory tests would be early morning. Gonadotropin levels and sex steroid levels should be checked in a laboratory with very sensitive assays appropriate for children.
13.
(E)
Turner syndrome. Turner syndrome in girls presents with primary ovarian failure because of atresia of the ovaries in fetal life. Many girls with Turner syndrome first present in early adolescence because of short stature and delayed puberty. In Kallmann syndrome, isolated gonadotropin deficiency and anosmia is found because of failure of the GnRH neurons and olfactory bulb to migrate properly. Craniopharyngioma and the subsequent treatment can lead to panhypopituitarism, and anorexia nervosa can lead to hypothalamic hypogonadism.
14.
(C)
Gonadal abnormality. Secondary hypogonadism is a result of disorders that decrease gonadotropin secretion. Lack of thyroid hormone has been shown to interfere with gonadotropin secretion. An abnormality in the gonad would lead to elevated gonadotropin levels.
15.
(C)
Right-sided cardiac defects. Girls with Turner syndrome usually present with short stature and delayed puberty because of primary ovarian failure. Occasionally, girls are diagnosed at birth because of puffy hands and feet, and a webbed neck because of lymphedema. They have a 45,XO karyotype (or a mosaic karyotype, ie, 45,XO/ 46,XX). Associated features include webbed neck, low posterior hairline, cubitus valgus, spooned nails, renal anomalies, and left-sided cardiac defects including coarctation of the aorta. Right-sided cardiac defects are found in Noonan syndrome, which has similar phenotypic findings as Turner syndrome with a normal karyotype. Girls with Noonan syndrome have normal ovarian function, but boys typically have cryptorchidism and abnormal Leydig cell function.
16.
(A)
Short stature. Klinefelter syndrome is the most frequent form of hypogonadism in males with an incidence of 1 in 500-1000 males. In all cases, seminiferous tubule function is impaired. Patients have variable Leydig cell function and thus can have testosterone levels from low to normal. Patients often have the onset of puberty at a normal age, but secondary sexual changes do not progress to the adult stage. Karyotype is 47,XXY, or variants including 48,XXXY, 49,XXXXY and male 46,XX. The typical phenotype includes tall stature with long arms and legs, small firm testes, small phallus, poor muscular development, language difficulties, and poor social adaptation.
17.
(D)
Bone age. The age at which children go into puberty varies widely. Bone age has been shown to be a better predictor of pubertal milestones than chronological age. Thus an 8-year-old girl with a bone age of 12 would be expected to be in puberty. Conditions that cause an advancement of bone maturation (such as undertreated congenital adrenal hyperplasia) can lead to precocious puberty.
18.
(B)
Advancement of bone maturation. The goals of therapy for delayed puberty include inducing the development of age-appropriate secondary sex characteristics, a growth spurt, and psychosocial benefits. Psychosocial concerns tend to be more pronounced in boys than girls because of societal pressures and can lead to low self-esteem and poor body image. If the therapy advances the bone maturation too quickly, children can have premature epiphyseal fusion and end up short as an adult.
 S
S
UGGESTED
R
EADING
Hughes IA. The testes: disorders of sexual differentiation and puberty in the male. In: Sperling MA, ed.
Pediatric Endocrinology.
3rd ed. Philadelphia, PA: WB Saunders; 2008:662-685.
Rosen DS, Foster C. Delayed puberty.
Pediatr Rev.
2001;22:309–315.
Rosenfield RL, Cooke DW, Radovick S. Puberty and its disorders in the female. In: Sperling MA, ed.
Pediatric Endocrinology.
3rd ed. Philadelphia, PA: WB Saunders; 2008:530-609.
Stafford DEJ. Delayed puberty. In: Radovick S, MacGillivray MH, eds.
Pediatric Endocrinology
,
A Practical Clinical Guide
. Totowa, NJ: Humana Press; 2003:383-397.
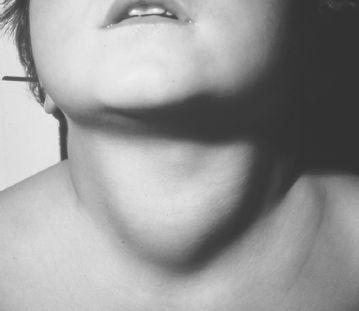
CASE 40: A 10-YEAR-OLD WITH A GOITER
A 10-year-old child is brought into your office for a routine school physical. On review of systems, the child has been complaining of fatigue but is doing well at school. The child is not taking any medications and has otherwise been healthy. There is a history of some type of thyroid problem in the maternal grandmother and paternal aunt. On physical examination you notice that the child has a goiter with no palpable nodules (see
Figure 40-1
).