Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis (136 page)
Authors: Mary A. Williamson Mt(ascp) Phd,L. Michael Snyder Md

BOOK: Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis
12.05Mb size Format: txt, pdf, ePub
Structural (e.g., diaphragmatic hernia, jejunal atresia, volvulus, intestinal malrotation) Peritonitis caused by GI tract perforation, congenital infection (e.g., syphilis, TORCH [
t
oxoplasmosis,
o
ther agents,
r
ubella,
C
MV, and
h
erpes simplex], hepatitis), meconium peritonitis
M1
gangliosidosis type I, I-cell disease, β-glucuronidase deficiency)
Immune (maternal antibodies reacting to fetal antigens [e.g., Rh, C, E, Kell])
PERITONITIS, ACUTE
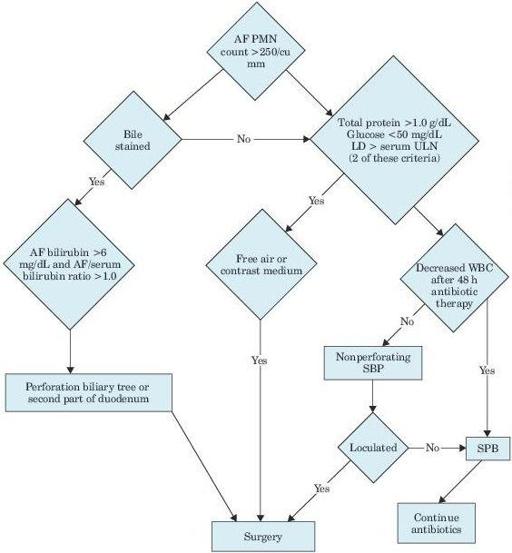
Figure 5–3
Algorithm for differentiating secondary from spontaneous bacterial peritonitis. AF, ascitic fluid; PMN, polymorphonuclear leukocytes; LD, lactate dehydrogenase; ULN, upper limit of normal; WBC, white blood cell; SBP, spontaneous bacterial peritonitis.
Other books
Assignment Unicorn by Edward S. Aarons
Contagious Lust by Snapper, Red, BlaQue, Essence
The Corpse Wore Cashmere by Sylvia Rochester
Good Intentions by Joy Fielding
Ghosts of Mayfield Court by Russell, Norman
The Shells Of Chanticleer by Patrick, Maura
The Nerdy Dozen #2 by Jeff Miller
Forged in Steele by Maya Banks
Dark Web (DARC Ops Book 2) by Jamie Garrett
Silent Witnesses by Nigel McCrery