Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis (1382 page)
Authors: Mary A. Williamson Mt(ascp) Phd,L. Michael Snyder Md

BOOK: Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis
13.86Mb size Format: txt, pdf, ePub
HIV has evolved into several groups: M, N, O, and P. Group M (“main”) is considered the pandemic strain and comprise most strains of HIV. Group O (“outlier”) represents far fewer strains from Cameroon, Gabon, and Equatorial Guinea. Group N (“non-M/non-O”) and group P are represented by very few isolates and have only been documented in Cameroon. Viruses from group M are subsequently divided into 10 distinct subtypes (A–J). HIV testing was originally developed to detect HIV subtype B, the most common subtype in the United States and Europe. The estimated frequency of non-B subtypes in the United States is approximately 2%. The CDC does not recommend routine testing for HIV-2 in settings other than blood centers.
Normal range:
Negative.
Use
17-1
)
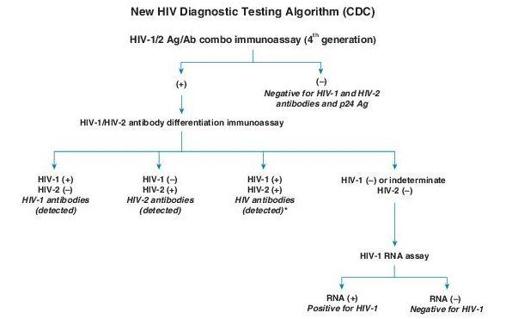
(+) = Reactive (or repeatedly reactive) test result, in accordance with manufacturer’s instructions
(–) = Nonreactive test result, in accordance with manufacturer’s instructions
Italics = Final interpretation; No further testing indicated for the specimen
*
Additional testing required to rule out dual infection with HIV-1/ HIV-2.
Figure 17–1
HIV diagnostic testing algorithm. (From Morbidity & Mortality Weekly Report. June 21, 2013, 62:490–494.)
Other books
The Cattleman (Sons of Texas Book 2) by Anna Jeffrey
The Poisons of Caux: The Hollow Bettle (Book I) by Susannah Appelbaum
His Texas Bride by Deb Kastner
Totlandia: Spring by Josie Brown
Born to Dance by June Tate
Monster: Made & Broken (A Mafia Bad Boy Romance) by Nora Ash
The World is Moving Around Me by Dany Laferriere
Signs of Love by Kimberly Rae Jordan
Time of the Eagle by Sherryl Jordan