Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis (211 page)
Authors: Mary A. Williamson Mt(ascp) Phd,L. Michael Snyder Md

BOOK: Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis
11.86Mb size Format: txt, pdf, ePub
Diffuse nontoxic (simple) goiter—relative deficiency of thyroid hormone
II. Nodular enlargement of the thyroid gland is seen in the following situations:
A. Benign solid nodule.
Hyperplastic (or colloid) nodule
B. Malignant tumors.
Papillary/follicular/anaplastic carcinomas arise from thyroid follicular epithelial cells. Papillary and follicular cancers are considered differentiated cancers, and patients with these tumors are often treated similarly despite numerous biologic differences. Most anaplastic (undifferentiated) cancers appear to arise from differentiated cancers.
Medullary carcinoma arises from calcitonin-secreting C cells and can occur in both sporadic and hereditary forms. The sporadic (noninherited) form accounts for 80% of cases and is usually unilateral. The hereditary form makes up 20% of the cases, is usually multicentric, and can be transmitted as a single entity and part of multiple endocrine neoplasia (MEN) types 2A and 2B, and familial non-MEN.
C. Multinodular goiter can present with or without thyrotoxicosis. A retrospective study showed that the risk of malignancy was similar in patients with multinodular goiter and one or more dominant nodules to the patients with solitary nodule. Therefore, a dominant nodule in a multinodular goiter should be evaluated as if it were a single nodule.
D. Simple cyst.
Who Should Be Suspected?
As mentioned earlier, thyroid nodules can be noted by the patient on self-examinations or by the physician on routine physical examinations. In addition, the presence of goiter or thyroid nodules should be suspected in patients with the following symptoms or signs.
1. Pain, pressure, or fullness in the neck
2. Hoarseness or change in voice
3. Trouble swallowing
6-3
)
1. Serum TSH should be measured in any patient with a goiter or nodules. It may be used as a first-line screening test. In multinodular goiter, TSH usually is in normal or low-normal range; it is rarely increased.
2. Calcitonin level is increased in virtually all patients with clinical medullary carcinoma. However, it is not cost-effective or necessary in patients without clinical suspicion due to rarity of the disease and high frequency of false-positive results.
3. Measurement of serum antithyroid peroxidase antibody and antithyroglobulin antibody levels may be helpful in the diagnosis of chronic autoimmune thyroiditis, especially if the serum TSH level is elevated.
4. Fine needle aspiration (FNA) biopsy of the nodule is the most time- and cost-efficient evaluation. The reported overall rates of sensitivity and specificity exceed 90% in iodine-sufficient geographic areas. FNA biopsy should be performed in any patient with a solitary or predominant nodule in a multinodular gland, unless the TSH is suppressed, implying autonomous function and, therefore, a low likelihood of malignancy.
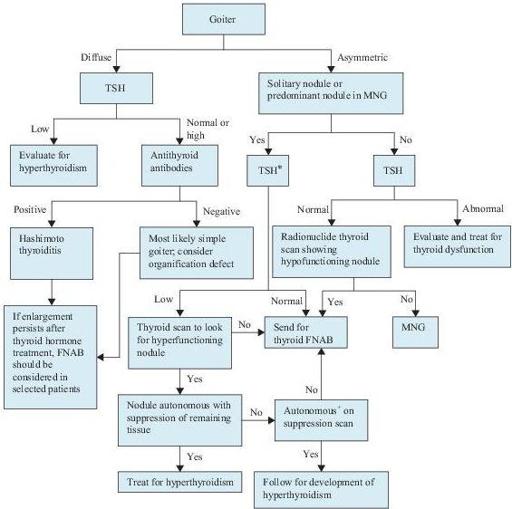
Figure 6–3
Algorithm for the diagnosis of goiter and thyroid nodules. *Include measurement of serum calcitonin if there is a family history of medullary cancer or multiple endocrine neoplasm, type 2 (MEN2).
+
Autonomy is defined as the ability to concentrate radioactive iodine despite TSH suppression. FNAB, fine needle aspiration biopsy; MNG, multinodular goiter; TSH, thyroid-stimulating hormone.
Other books
The Early Stories by John Updike
Fancy Pants (Only In Gooding Book #1) by Hake, Cathy Marie
Free Lunch by David Cay Johnston
FALL (The Senses) by Paterson, Cindy
Murder Close to Home by Elizabeth Holly
Survivors by Rich Goldhaber
Cry in the Night by Hart, Carolyn G.
Harajuku Sunday by S. Michael Choi
Desired Affliction by C.A. Harms
Moral Imperative by C. G. Cooper