Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis (236 page)
Authors: Mary A. Williamson Mt(ascp) Phd,L. Michael Snyder Md

BOOK: Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis
6.49Mb size Format: txt, pdf, ePub
Cystine stones are rare, occurring in patients with homozygous congenital familial cystinuria, and characterized by bilateral obstructive staghorn calculi with associated renal failure.
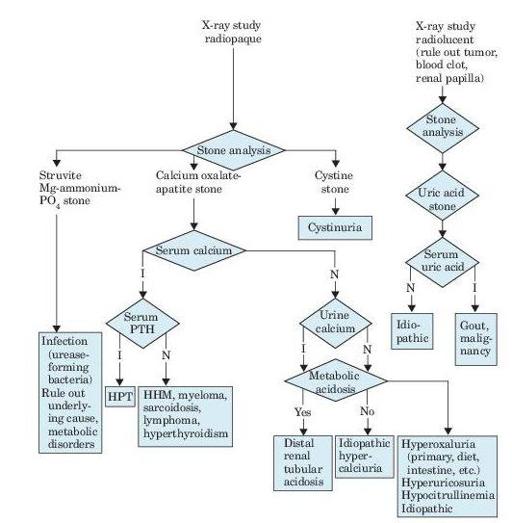
Figure 7–1
Algorithm for diagnosis of renal calculi, as revealed by flank pain, renal colic, hematuria, fever, and urinalysis findings. I, increased; N, normal; PTH, parathyroid hormone; HPT, hyperparathyroidism; HHM, humeral hypercalcemia of malignancy.
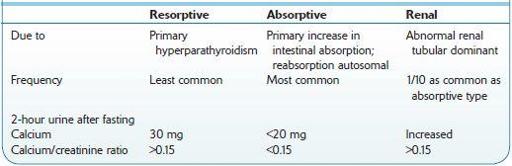
Table 7-1 Comparison of Types of Idiopathic Hypercalciuria
Who Should Be Suspected?
The waves or paroxysms of pain usually last 20–60 minutes and is related to the passage of the stone down the ureter and the associated ureteral spasm.
Other books
El juez de Egipto 2 - La ley del desierto by Christian Jacq
Tek Kill by William Shatner
The Wind Chill Factor by Thomas Gifford
Darla's Story by Mike Mullin
Heart Fortune (Celta) by Owens, Robin D.
Fortune's fools by Julia Parks
At Any Price (Gaming The System) by Aubrey, Brenna
You Don't Even Know Me by Sharon Flake
Mercy Killing (Affairs of State Book 1) by Johnson, Kathryn
Lucky Me by Saba Kapur