Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis (522 page)
Authors: Mary A. Williamson Mt(ascp) Phd,L. Michael Snyder Md

BOOK: Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis
12.18Mb size Format: txt, pdf, ePub
TABLE 12–1. Staging of Acute Kidney Injury
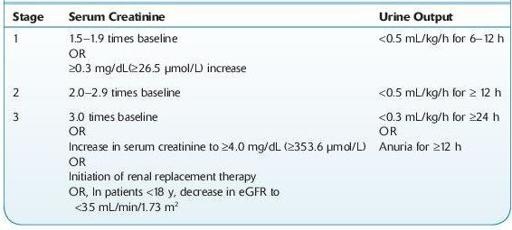
eGFR, estimated glomerular filtration rate.
Source: Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group.
KDIGO clinical practice guideline for acute kidney injury.
Kidney Int.
2012;2(Suppl):1–138.
Who Should Be Suspected?
Patients with AKI present in a variety of ways:
Patients with symptoms suggestive of uremia. The term uremia describes the clinical syndrome associated with retention of the end products of nitrogen metabolism due to severe reduction in renal function. It can be a consequence of either acute or chronic renal disease.
12-1
). Microscopic examination is normal in most cases of prerenal disease. The presence of RBC casts or dysmorphic RBCs indicates glomerular disease, whereas finding cellular debris or granular casts suggests ischemic or nephrotoxic AKI. Urine specific gravity is of limited value in establishing the etiology of AKI.
Other books
Necromancer's Revenge by Emma Faragher
Fortress of Spears by Anthony Riches
Vampires Seduction #1 (The Paranormal Town Romance Series) by Tasha Scott
Lady of the Lake by Elizabeth Mayne
Called by the Bear 4-6 by V. Vaughn
Is He Or Isn't He? by John Hall
A Need To Kill (DI Matt Barnes) by Michael Kerr
Strong and Sexy.2 by Jill Shalvis
Rolling Thunder by John Varley
Hell's Diva by Anna J.