Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis (543 page)
Authors: Mary A. Williamson Mt(ascp) Phd,L. Michael Snyder Md

BOOK: Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis
12.3Mb size Format: txt, pdf, ePub
Focal nephritic: generally associated with inflammatory regions in less than one half of glomeruli. Patients often present with asymptomatic hematuria and proteinuria.
Causes
Renal: can be postinfectious (due to certain nephritogenic strains after streptococcal, staphylococcal, or pneumococcal infections, mumps, measles, chickenpox, hepatitis B and C) or due to MPGN or anti–glomerular membrane disease.
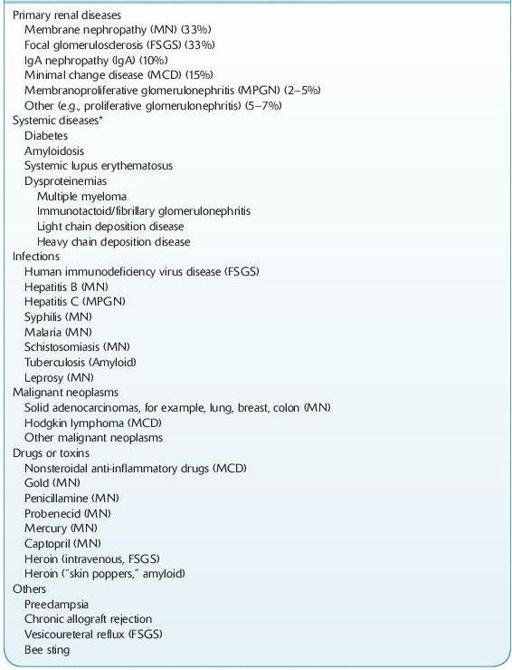
NEPHROTIC SYNDROME
This syndrome presents as heavy proteinuria, hypoalbuminemia, hyperlipidemia, lipiduria, and edema.
12-5
).
TABLE 12–5. Major causes of Nephrotic Syndrome
Other books
Come Into The Light by O'Rourke, Stephen
Ginny Gold - Early Bird Café 02 - Deadly Surprise by Ginny Gold
Cyndi Lauper: A Memoir by Lauper, Cyndi
Breathless (The Breathe Series) by Brookes, Rachel
Twelve Truths and a Lie by Christina Lee
First and Last by Rachael Duncan
Blood Hunt by Butcher, Shannon K.
Still Not Dead Enough , Book 2 of The Dead Among Us by Doty, J. L.
The Unexpected Coincidence by Amelia Price