Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis (59 page)
Authors: Mary A. Williamson Mt(ascp) Phd,L. Michael Snyder Md

BOOK: Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis
11.08Mb size Format: txt, pdf, ePub
Who Should Be Suspected?
A transient, complete loss of consciousness and postural tone with spontaneous complete recovery without sequelae is likely to be syncope as opposed to a nonsyncopal event with apparent loss of consciousness. Differential of the latter includes seizure, hemorrhage, pulmonary embolism, subarachnoid hemorrhage, and metabolic (hypoglycemia/hypoxia) (Figure
3-3
).
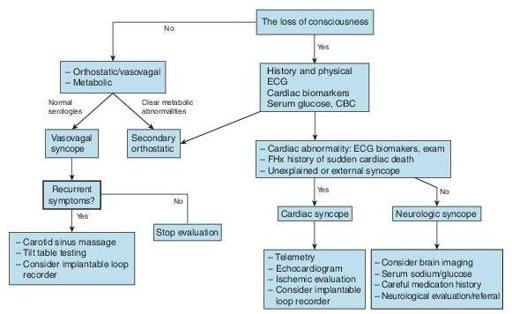
Figure 3–3
Evaluation of syncope.
Plasma BNP
may aid in distinguishing cardiac from noncardiac syncope but is not yet endorsed by professional society guidelines. A large prospective study (released after most current guidelines) utilizing a risk-stratification admission algorithm if any of the following were present: BNP ≥300 pg/mL, bradycardia ≤50 bpm, fecal occult blood, anemia with ≤9 g/dL, chest pain, Q waves on ECG, or oxygenation saturation ≤94% had a sensitivity of 87% and specificity of 66% with negative predictive value of 98.5%.
electrocardiogram
should be performed in all patients with syncope and is central to risk stratification of patients with syncope. The presence of highrisk features should dictate hospital admission and further evaluation, not the diagnosis of syncope. ECG high-risk features include bifascicular block, QRS ≥0.12 seconds, Mobitz I second-degree AV block, sinus bradycardia (≤50 bpm), or sinus pause ≥3 seconds without chronotropic medications, evidence of preexcitation (Wolf-Parkinson-White syndrome), long or short QT intervals, Brugada syndrome (RBBB with ST elevation V1–V3), and Q waves. Clinical high-risk features that require hospitalization are the presence of cardiac structural disease, family history of sudden cardiac death, severe anemia, palpitations at the time of syncope, exertional syncope, electrolyte disturbances, and severe comorbidities.
Other books
Guardian of Justice by Carol Steward
Street Gang by Michael Davis
The Destiny of Nathalie X by William Boyd
Without Fail by Lee Child
The Empress' Rapture by Trinity Blacio
Me Before You by Moyes, Jojo
A Shattered Wife by Diana Salyers
It Happened on the Way to War by Rye Barcott
The Other Woman by Eve Rabi