Connectome (7 page)
Authors: Sebastian Seung

As I lifted the sheets that covered the boy, I was stunned to find that his left leg was half-missing; it had been amputated right below the knee after being run over by a car. I suddenly realized that the child's pain came from a part of his body that no longer existed. Outside the ward I heard the surgeon saying, “It was not him speaking; it was his phantom limb.”
Â
Modern methods of amputation were invented in the sixteenth century by Ambroise Paré, who perfected his art as a surgeon for the French army. Paré was born at a time when surgery was performed by barbers, because it seemed like a crude act of butchery
too lowly for physicians. Working on the battlefield, Paré learned how to tie off large arteries
to prevent amputees from bleeding to death. He eventually earned employment with several French kings and a place in the history books as the “father of modern surgery.”
Paré was the first to report that amputees complained of an imaginary limb still attached to the body where the real limb used to be. Centuries later, the American physician Silas Weir Mitchell coined the term
phantom limb
to describe the same phenomenon in Civil War soldiers. His many case studies established that phantom limbs are the rule, not the exception. Why had they gone unremarked for so long?
Before the surgical innovations of Paré, very few people survived amputation, and the complaints of those who did may have been dismissed as mere delusions. But far from being irrational, amputees are well aware that the phantom is not real,
and because its sensations are usually painful, they beg doctors to make it go away.
Along with naming it, Mitchell proposed a theory to explain the phenomenon. He suggested that irritated nerve endings
in the stump were sending signals to the brain, which interpreted them as sensations from the missing limb. Inspired by the theory, some surgeons tried amputating the stump, but this didn't help.
Today many neuroscientists believe a different theory: Phantom limbs are caused by a remapping of the cortex.
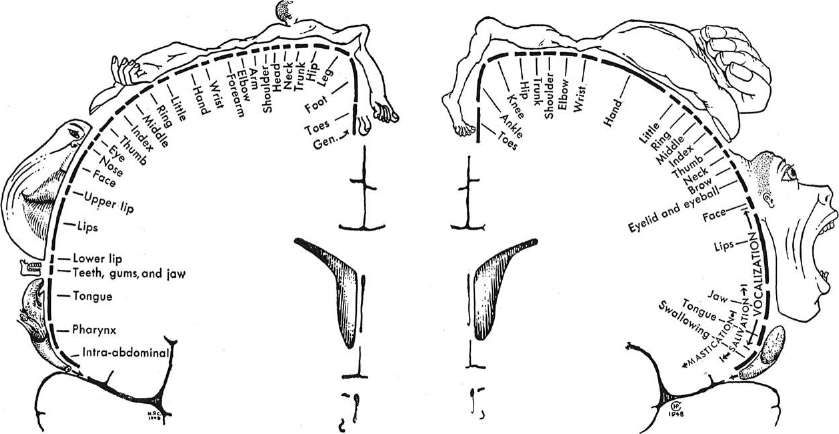
The reorganization is not of the entire cortex; it's thought to be confined to a particular area. We previously learned about area 4, the strip in front of the central sulcus that controls movement. Just behind the central sulcus is area 3, which is involved in the bodily sensations of touch, temperature, and pain. In the 1930s the Canadian neurosurgeon Wilder Penfield mapped both areas in his patients by using electrical stimulation. After opening the skull to expose the brain for epilepsy surgery, Penfield applied his electrode to different locations in area 4. Each stimulation caused some part of the patient's body to move. Penfield drew the correspondence between area 4 locations and body parts (Figure 12, right), calling the map a “motor homunculus.” (
Homunculus
is from the Latin for “little human.”) Likewise, after each stimulation of area 3, the patient reported feeling a sensation in some part of the body. Penfield mapped the “sensory homunculus” in area 3 (left), and it looked similar to the motor one. Both ran in parallel along opposite banks of the central sulcus. (Roughly speaking, these maps represent vertical planes passing through the brain from ear to ear. The plane of the sensory map is just behind the central sulcus, and that of the motor map just in front. Only the outer border is cortex; the rest is the interior of the cerebrum.)
Â
 Â
Â
Â
Figure 12. Functional maps of cortical areas 3 and 4: the “sensory homunculus”
(left)
and the “motor homunculus”
(right)
Â
The face and hands dominate the maps, even though they are small parts of the body. Their cortical magnification reflects their disproportionate importance in sensation and movement. Could the sizes of their territories be changed by amputation, which suddenly reduces the importance of a body part to zero? Using such reasoning, the neurologist V. S. Ramachandran
and his collaborators have proposed that phantom limbs are caused by remapping of area 3. If the lower arm is amputated, its territory in the sensory homunculus loses its function. The surrounding territories, dedicated to the face and upper arm, encroach upon the nonfunctional one by advancing their borders. (You can see the adjacencies in Penfield's drawing.) These two intruders start to represent the lower arm as well as their original body parts, giving the amputee the sensation of a phantom limb.
According to the theory, the remapped face territory should represent the lower arm as well as the face. Therefore Ramachandran predicted that stimulation of the face would cause sensations in the phantom limb. Indeed, when he stroked the face of an amputee
with a Q-tip, the patient reported feeling sensations not only in his face but also in his phantom hand. The theory likewise predicts that the remapped upper-arm territory should represent the lower arm as well as the upper arm. When Ramachandran touched the stump, the patient felt sensations in both the stump and his phantom hand. These ingenious experiments strikingly confirmed the theory that amputation caused remapping of area 3.
Â
Ramachandran and his collaborators used technology no more advanced than a Q-tip. In the 1990s an exciting new method of brain imaging was introduced. Functional MRI
revealed every region's “activity,” or how much that part of the brain was being used. By now the images of functional MRI (fMRI) are familiar from their frequent appearance in the news media. They are usually shown superimposed on regular MRI images. The black-and-white MRI image shows the brain, and laid on top are the colored blotches of the fMRI image, which indicate the active regions. You can always recognize fMRI+MRI as “spots on brains,”
while MRI is just brains.
Researchers imaged volunteers while they performed mental tasks in the laboratory. If a task activated a region, causing it to “light up” in the image, that was a clue to the region's function. Neurology had always been hampered by the accidental nature of brain lesions, but fMRI enabled precise and repeatable experiments on localization of function. Brodmann's map became indispensable as researchers worked hard to assign functions to each of its areas. The boom in scientific papers spurred many universities to invest large sums of money in fMRI machines, or “brain scanners.”
Researchers also repeated Penfield's mapping of the sensory and motor homunculi. They observed which locations in area 3 were activated by touching parts of the body, and which locations in area 4 were activated when the subject moved parts of the body. It was thrilling to reproduce Penfield's maps with fMRI rather than his crude method of opening up the skull. Researchers also studied remapping, verifying Ramachandran's claim of a downward shift of the face representation in area 3 of amputees. As the theory predicted, the shift occurred
only in those amputees who experienced phantom limb pain, not in pain-free amputees.
Amputation may not be injury to the brain, but it's still a highly abnormal kind of experience. Do brains remap in more normal forms of learning? Violinists and other string musicians use the left hand to finger the strings of their instruments. Studies show enlargement of the left-hand representation
within area 3, which is likely due to extensive musical practice. It's impressive that fMRI can not only assign functions to Brodmann areas but also resolve fine changes within a single area. This research is far more sophisticated than studies of total brain size like Galton's. It is bound to tell us more interesting things about cortical remapping, and it may even be useful for understanding crippling disorders
of movement that seem to be caused by too much practice. Such disorders, known as focal dystonias,
have tragically ended the careers of brilliant musicians.
Explaining learning in terms of the expansion of cortical areas or subareas, however, is still in the spirit of phrenology. It's not so different in concept from the studies of cortical thickening, and the correlations are still statistically weak. The approach may be powerful, but it has limitations. For example, studies of Braille readers also show an enlarged hand representation. The remapping approach cannot easily distinguish between learning violin and Braille,
which are two very different skills. And even if this particular problem can be solved, the general difficulty will remain.
Researchers have one other way of studying changes in the brain, which does not depend on the concept of remapping. Using fMRI, they have attempted to find differences in the level of activation of brain regions. For example, they have reported lower activation of the frontal lobe in schizophrenics
performing certain mental tasks. At the moment such correlations are statistically weak, but this intriguing line of research may well tell us much about brain disorders
and possibly lead to superior methods of diagnosing them.
At the same time, fMRI studies may have a fundamental limitation. Brain activation changes from moment to moment, roughly as quickly as thoughts and actions change. To find the cause of schizophrenia, we must identify some brain anomaly that is constant. Suppose that your car starts to shake whenever you drive faster than 30 miles per hour and turn the steering wheel to the right. This behavior is intermittent, so it's only a symptom. It's caused by something wrong with your car at a more basic level. Noticing symptoms is crucial, but it's only the first step toward identifying the underlying cause.
Â
Why are we still trying to use phrenology to explain mental differences? It's not because the strategy is good. It's because we have failed to come up with a better one. Do you know the joke about the policeman who comes upon a drunk crawling on the ground near a lamppost? The drunk explains, “I lost my keys around the corner.” The policeman asks, “Well, why don't you search over there?” The drunk replies, “I would, but there's more light under the lamppost.” Like the drunk who works with what he's got, we know that size reveals little about function, but we look at it anyway because that's what we can see with existing technologies.
To understand the failings of phrenology, can we compare with a more successful example of relating function to size? Instead of investigating whether brainy people are smarter, let's ask whether brawny people are stronger. The size of a muscle can be measured via MRI, and its strength
with a machine that looks like one in the weight room at your health club. Researchers have found correlation coefficients
ranging from 0.7 to 0.9, which is much stronger than the correlation between brain size and IQ. Muscle size accurately predicts strength, just as we'd expect.
Why are size and function so closely related for muscles but not for brains? Think of a muscle as operating like a factory in which all workers do the same thing. If every worker singlehandedly performs all the steps required for making an entire widget, doubling the size of the workforce will double the factory's output of widgets. Likewise, every fiber of a muscle performs the same task. All the fibers are lined up in parallel, and all pull in the same direction. Their contributions to the force are additive (you can simply add them together to get the total), so a muscle with more fibers should be stronger.
Now consider a factory with a more complex organization. Each worker performs a different task, like fastening a screw or welding a joint. To make even a single widget, all the workers must cooperate. Economists say that such division of labor is efficient because specialization allows each worker to become highly skilled at each task. However, doubling the number of workers will likely fail to double the output of widgets. It's not easy to integrate the new workers into the existing organization in a way that increases output. In fact, adding more workers could even reduce output by disrupting the workflow. As Brooks' Lawâa maxim of software engineersâputs it, “Adding more programmers to a late software project makes it later.”
The brain works like the more complex factory. Each of its neurons performs a tiny task, and they cooperate in intricate ways to carry out mental functions. That's why performance depends less on the number of neurons and more on how they are organized.
The factory analogy explains the limitations of phrenology. Can it also explain remapping? The American neuropsychologist Karl Lashley believed that mental functions were widely distributed across the cortex, and charged that most of the boundaries of Brodmann's map
were figments of the imagination. Nevertheless, this archenemy of localizationism could not completely deny the experimental evidence in its favor. In 1929 he countered with his doctrine of cortical
equipotentiality.
Lashley granted that every cortical area is dedicated to a specific function, but every area also has the
potential
to assume some other function, he claimed.
Returning to our imaginary factoryâthe more complex oneâlet's suppose that a worker is reassigned to a new task. The initial clumsiness will eventually give way to proficiency. Workers may be specialized, but they are also equipotential. When provided with new inputs, they can change their functions.