Connectome (6 page)
Authors: Sebastian Seung

Most of us are convinced that minds differ because brains differ; so far, however, there is little proof. The phrenologists tried to find evidence by examining the sizes of the brain and its regions, but only recently has MRI provided the technological means to execute their strategy properly. Neo-phrenology has confirmed that mental differences are statistically related to brain size, by revealing weak correlations in groups of people, but the differences do not accurately predict genius, autism, or schizophrenia in individuals.
I wish neuroscience were winning its game more convincingly. The stakes are high. Discovering neuropathologies for autism and schizophrenia could aid the search for therapies. Understanding what makes a brain intelligent could help us devise better teaching methods or other tools to make people smarter. We don't just want to understand the brain. We want to change it.
God, grant me the serenity
To accept the things I cannot change
Courage to change the things I can
And wisdom to know the difference.
Â
The serenity prayer has been adopted by Alcoholics Anonymous and other organizations that help members recover from addiction. It reveals why the brain fascinates people so much: They are always hoping to change it. Just stroll through the self-help section of your local bookstoreâyou'll see hundreds of titles on how to drink less, quit drugs, eat right, manage money, discipline your kids, and save your marriage. All these things seem possible, but they are difficult to achieve.
Certainly normal, healthy adults would like to change their behaviors, but this goal is even more critical for those with mental disabilities and disorders. Can a young adult ever be cured of schizophrenia? Can a grandparent learn to speak again after a stroke? And we all want our schools and our childrearing to mold young minds for the better. Can we improve the way this is done?
The Serenity Prayer asks for courage and wisdom about change. Wouldn't it be better to have answers from neuroscience as well? After all, changing the mind is ultimately about changing the brain. But neuroscience can never aid the quest for self-improvement without answering a more fundamental question: How exactly does the brain change when we learn to behave in a new way?
Parents marvel at the speed of their babies' development, excitedly celebrating every new action or word as a wondrous occasion. The infant brain grows rapidly,
reaching close to adult size by two years of age. This suggests a simple theory: Perhaps learning is nothing more than brain growth, and children can be made smarter by enhancing this growth.
This theory goes back yet again to the phrenologists. Johann Spurzheim argued that mental exercise could enlarge cortical organs, much as muscles bulk up after physical training. Based on this theory, Spurzheim went on to develop an entire philosophy of education
for both children and adults.
More than a century passed before his theory was finally tested scientifically. By that time, psychologists had invented a way of studying the effects of stimulation on the animal mind. Laboratory rats were placed in two different environments, one dull and the other “enriched.” In the dull cage, a solitary rat lived with food and water containers as the only decoration. In the enriched cage, many rats lived together in a group and were provided daily with new toys. By running the rats through simple mazes,
researchers found that the enriched rats were smarter. Presumably their brains were different, but exactly how?
In the 1960s Mark Rosenzweig
and his colleagues decided to find out. Their method was startlingly simple: They weighed the cortex. It turned out that the enriched cage slightly enlarged the cortex on average. This was the first demonstration that experience causes the brain's structure to change.
You might not be surprised. After all, what about those MRI studies showing that London taxi drivers, musicians, and bilinguals have enlarged brain regions? Once again we must be careful not to read too much into statistical findings. The MRI studies showed correlation, but they did not prove causation.
Did driving a taxi, playing a musical instrument, and speaking a second language
cause
the brain to enlarge, as in Spurzheim's theory? Causation could be claimed if the brains of musicians and non-musicians were the same before musical training, and only became different afterward. But since the MRI study only collected data about “after,” it cannot rule out an alternate interpretation: Perhaps some people are born with a brain enlargement that endows musical talent, and these gifted people are more likely to become musicians. Enlarged brains cause musical training, not the other way around.
Musicians may be selected on the basis of innate talent by music teachers and competitions. And musicians may be self-selecting, since people generally prefer activities at which they excel. This sort of problem, known as
selection bias,
complicates the interpretation of many statistical studies. Rosenzweig eliminated selection bias by
randomly
installing some rats in the enriched cage and others in the dull cage. This ensured that the two groups of rats started out statistically identical, enabling him to interpret any differences after the cage experience as having been caused by it.
For an even more direct demonstration of causation, one can use MRI to compare human brains before and after an experience. In this way, researchers found that learning to juggle balls
thickened the cortex in the parietal and temporal lobes. And intensive study for exams
caused the parietal cortex and the hippocampus to enlarge in medical students.
These results are impressive, but they are still not what we want. It is not enough to show that experience changes the brain. We also want to know whether the change is the cause of the improved performance. To understand why proof is still lacking, consider the following analogy. Imagine that musical training causes musicians to become more obese by forcing a sedentary lifestyle of practicing all day long. It would be wrong to conclude that obesity causes their improved musical performance. Similarly, showing that musical training enlarges the brains of musicians does not prove that this growth causes them to play their instruments better.
Rosenzweig showed that living in the enriched cage made rats smarter and also thickened their cortex. He did not prove, however, that it was the thickening that caused the improvement in intelligence. In fact, this seems unlikely, given what we know about the functions of cortical regions. The frontal lobe is thought to be important for skills like maze-running, but it showed little or no increase in size. The occipital lobe, which is responsible for visual perception, showed the largest increase.
In the end, we cannot equate cortical thickening with learning. We can say only that these two phenomena are correlated. Furthermore, the correlation is weak, once again revealed only by averages over groups. Cortical thickening is not a reliable predictor of learning in individuals.
Â
Perhaps studying maze-running or juggling is the wrong approach. Maybe we should study more dramatic changes. Immediately after a stroke, for example, a patient usually experiences weakness or paralysis and may also lose speech and other mental abilities. Many patients improve dramatically over the next few months. What happens to the brain during recovery? Research on this question is of clear practical importance, as it could help us develop better therapies.
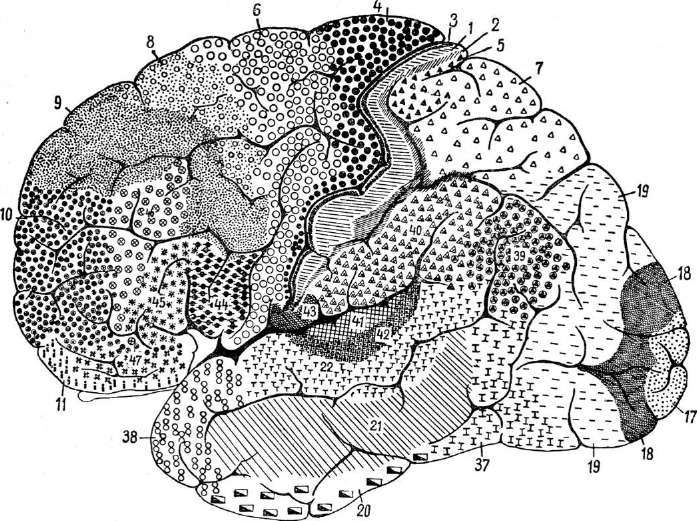
Strokes are caused by blocked or leaking blood vessels that damage the brain. The symptoms often indicate which side of the brain has been damaged. If patients struggle to control one side of the body, as is frequently the case, it means that the opposite side of the brain has been damaged, because each side of the brain controls muscles on the opposite side of the body. Neurologists can sometimes further pinpoint the affected brain region. To describe the location of cortical injury, a neurologist may specify a lobe or, if more precision is needed, a particular fold in a lobe. The folds have fancy-sounding names like “superior temporal gyrus,” which means the uppermost fold in the temporal lobe. Alternatively, a cortical area may be specified by a number rather than a name, using a map published by the German neuroanatomist Korbinian Brodmann
in 1909 (see Figure 11). In this book I will use the term
area
to mean a subdivision of Brodmann's map, and
region
to refer to any subdivision of the brain.
Â
 Â
Â
Â
Figure 11. Brodmann's map of the cortex
Â
Loss of movement after a stroke can result from damage to areas 4 and 6. Area 4 is the rearmost strip of the frontal lobe, just in front of the central sulcus, and area 6 is in front of area 4. Both are known to be important for control of movement. Language, too, is commonly impaired by stroke. That's a sign of damage to Broca's region (areas 44 and 45) or Wernicke's region (the back end of area 22), both in the left hemisphere.
Friends and family desperately want to know how much recovery is possible. Will Grandpa walk again? Will he talk? Movement tends to improve over time, but not much more after three months.
Language also recovers most rapidly during the first three months, though it can continue to improve for months or years afterward. Neurologists know the three-month mark is important, but they do not know exactly why. More fundamentally, they don't know exactly what changes are taking place inside the brain as the patient recovers.
Obviously, the affected brain region might recover part or all of its function. But some cells near the malfunctioning blood vessel actually die, causing irreversible damage. Could the spared regions take over for the damaged region? Imagine that one of the players on a soccer team suffers an injury and is carried in agony off the playing field. There are no substitute players sitting on the bench, so the shorthanded (or shortfooted) team now plays worse. But as the game proceeds, the remaining players may adapt to the situation. If their comrade played in an attacking position before the injury, the defenders might compensate by starting to double as attackers.
So this is an important question: Can a cortical area acquire a new function after brain injury? There is some evidence for this after stroke,
but stronger confirmation comes from cases of brain damage in early life. The disorder of epilepsy is defined by repeated spontaneous “seizures,” or episodes of excessive neural activity. Children with very frequent and debilitating seizures are sometimes treated by removing one hemisphere
of the cerebrum entirely. This is one of the most radical neurosurgical procedures, and it's astonishing that most children recover very well from it. Afterward they walk and even run,
though movements of the hand on the opposite side are impaired. Their intellectual abilities are generally intact, and can even improve after surgery if the seizures are successfully eliminated.
One might argue that the recovery after hemispherectomy is not so surprising. Perhaps it's like losing a kidney. The remaining kidney need not do anything different; it just performs more of the same. But remember that some mental functions are lateralized, so the left and right sides of the brain are not equivalent. Because the left hemisphere specializes in language, its removal almost invariably leads to aphasia in adults. This is not true for children; linguistic functions migrate to the right hemisphere,
demonstrating that cortical areas can indeed change their functions.
Given what we know about localization, it's not surprising that neurologists can guess the location of brain injury from the symptoms. Here's the surprising “yes, but”: There may be a map dividing the cortex into areas with distinct functions, but the map is not fixed. The injured brain can redraw it.
Â
The remapping of the cortex seen after stroke or surgery is more dramatic than the thickening reported by the neo-phrenologists. Can remapping also happen in healthy brains? Once again, insight can be gained from cases of severe injuryâbut to the body, not the brain. The following passage comes from an article by the neuroscientist Miguel Nicolelis
:
Â
One morning in my fourth year of medical school, a vascular surgeon at the University Hospital in São Paulo, Brazil, invited me to visit the orthopedics inpatient ward. “Today we will talk to a ghost,” the doctor said. “Do not get frightened. Try to stay calm. The patient has not accepted what has happened yet, and he is very shaken.”
A boy around 12 years old with hazy blue eyes and blond curly hair sat before me. Drops of sweat soaked his face, contorted in an expression of horror. The child's body, which I now watched closely, writhed from pain of uncertain origin. “It really hurts, doctor; it burns. It seems as if something is crushing my leg,” he said. I felt a lump in my throat, slowly strangling me. “Where does it hurt?” I asked. He replied: “In my left foot, my calf, the whole leg, everywhere below my knee!”