Craving (26 page)
Authors: Omar Manejwala

According to Marlatt, when alcoholics are exposed to a high-risk situation, if their responses are ineffective, then their confidence in themselves is diminished, they drink, and then they experience a twist in their thinking (a cognitive distortion) called the abstinence violation effect and are more likely to drink again. The therapies that Marlatt and others who follow him have developed are designed to interrupt all aspects of this cascade and restore the person’s sense of efficacy and the cognitive and behavioral tools in their toolbox.
FIGURE 1
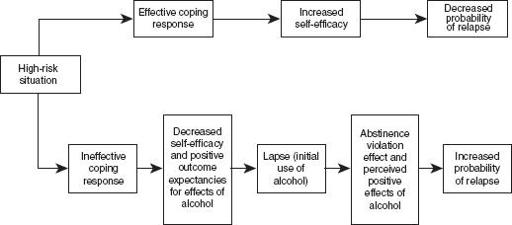
The diagram above shows how this works, and it makes a lot of sense.
125
Craving researchers have tested components of this model and found that it seems to hold up; in other words, the model does a fairly good job of explaining what happens when alcoholics cope effectively with risky situations and what happens when they don’t. According to this model, self-efficacy is the key to decreasing the probability of relapse.
Unfortunately, however, this seems to be at odds with Twelve Step philosophies. That wouldn’t be a big deal if Twelve Step programs weren’t so effective at helping many people get and stay sober. However, these programs
are
effective, and a central tenet of their system appears to be that efficacy comes from a higher power and that the self (or, more precisely, the
ego
) is actually the source of the problem. Twelve Step programs de-emphasize the importance of self and suggest that a person himself cannot generate robust thinking to prevent the initiation of substance use.
126
How can we resolve this apparent discrepancy? Which is it? Do alcoholics stay sober because of self-efficacy and learning new responses to high-risk situations à la Marlatt? Or do they stay sober because of admitting that they are powerless and accepting a higher power? These views are so opposed that the treatment field has not, in most cases, successfully resolved them. Instead, the field of addiction treatment has been polarized, with Twelve Step camps over here and cognitive-behavioral therapists over there, and “never the twain shall meet.” Although there are many exceptions, the trend has been for academics to be on the cognitive (or related) side, and nonacademics to be more Twelve Step biased.
The problem is not, however, simply a theoretical one or simply academic. Patients have suffered from the confusion and mixed messaging. After all, AA and other Twelve Step programs are based on the idea that a higher power can do what the individual cannot. Since many patients who enroll in treatment programs that espouse Marlatt’s approach will learn that self-efficacy is paramount to sobriety, their success may be undermined when they attend Twelve Step meetings and learn that the self is the problem and that only a higher power can keep them sober. I have been observing this dynamic for over a decade, and I can tell you that it is the source of much confusion, heartache, and even relapse.
Part of the confusion is over the term “self-efficacy.” The term “self” is both unnecessary and unnecessarily confusing. If we think of this as simply efficacy (rather than self-efficacy), much of the debate dissolves. Long-sober Twelve Step program members describe an unshakable faith that their participation in these programs will produce recovery. They know the Twelve Step program works. This sense of efficacy (although not exactly
self
-efficacy) drives their results in just the way Bandura and Marlatt predicted. True, they attribute their success to a power greater than themselves. Most, however, accept the notion that the power resides deep within themselves, although they emphasize that it is not the same as themselves.
127
Seen this way, Marlatt’s diagram is highly consistent with Twelve Step views, including the experience that a series of actions (the Steps), when taken, render the sufferer able to cope effectively with high-risk situations.
Another difference between talk therapies for addictive disorders and Twelve Step methodologies (leaving aside the obvious difference that Twelve Step programs are not therapy, although there are therapies that are specifically designed to facilitate Twelve Step participation) is that, in general, Twelve Step programs emphasize that they are designed to help those people who want to stop using alcohol (or the drug or other problem behavior). True, many people attend Twelve Step meetings before they are ready to stop (and that can often be helpful for some ambivalent people), but the programs are generally pretty clear about who they are designed to help—those who want it. Consider these lines from the book
Alcoholics Anonymous,
fourth edition:
“We are assuming, of course, that the reader desires to stop.” (p. 34)
“If you have decided you want what we have and are willing to go to any lengths to get it—then you are ready to take certain steps.” (p. 58)
Cognitive therapies and similar methods (including one called Motivational Enhancement Therapy) can be used for people who are not yet ready to stop. Or, simply put, treatment is about
dis
-covery and Twelve Step programs are about
re
-covery. So another key difference between these methods is the appropriate target population.
Yet another source of disagreement (or confusion) stems from the erroneous notion that Twelve Step programs tell you that you cannot think your way out of a drink (or a drug, or an addictive behavior), whereas cognitive methods such as Marlatt’s emphasize thinking (and improving the thinking process, if you will, via certain therapies) as a critical solution to high-risk situations. Well, which is it? Can you think your way to sobriety or can’t you? What is the role of thinking, and which camp is correct? Once again, although many in the field haven’t been able to see this clearly, the views aren’t really so opposed. In fact, Twelve Step programs emphasize the importance of thinking, once the dysfunctional thinking patterns have been addressed using the Twelve Steps:
On awakening let us think about the twenty-four hours ahead. We consider our plans for the day. Before we begin, we ask God to direct our thinking, especially asking that it be divorced from self-pity, dishonest or self-seeking motives. Under these conditions we can employ our mental faculties with assurance, for after all God gave us brains to use. Our thought-life will be placed on a much higher plane when our thinking is cleared of wrong motives.
128
In other words, both the cognitive approach to managing cravings and the Twelve Step methods emphasize that dysfunctional thinking (described in
Alcoholics Anonymous
as mental obsession, delusion, or wrong-motive thinking) drives alcoholic behavior and that transformative experiences are required to address that. In his later years, Marlatt became involved in developing mindfulness-based therapies to reduce cravings and substance use, which are very closely related to Twelve Step approaches.
I don’t mean to suggest that these philosophies are identical—they aren’t at all. Twelve Step programs emphasize the absolute importance of recognizing that there is a power greater than the individual and the importance of relying on that power in everything they do. Cognitive and related therapies emphasize the absolute importance of changing the way we think, through exercises that force us to examine and alter distortions in the conclusions about the facts of our experience. My point is that they really aren’t mutually exclusive and that more could be done for people who benefit from cognitive methods to help them incorporate Twelve Step programs into their recoveries without creating such a drastic (and destructive) either/or. This is important, because much of the psychosocial support available to people who suffer from cravings can be found in Twelve Step fellowships, and it can be much easier to access the key ingredients of successful recovery by utilizing these programs.
The bottom line is this: in the throes of addictive disease, and in the midst of craving, people will not always be able to rely on their brains to help them avoid succumbing to their urges. They may
sometimes
be able to use their thinking to help them, but for anyone who wants consistent success, something more is needed. Their thinking needs to change;
they
need to change. That requires actions of the type that I’m describing in this book.
…
Notes
1
. John M. Harlow, “Recovery from the Passage of an Iron Bar through the Head,”
History of Psychiatry
4, no. 14 (1993): 274–81.
2
. J. P. Brasil-Neto, A. Pascual-Leone, J. Valls-Sole, L. G. Cohen, and M. Hallett, “Focal Transcranial Magnetic Stimulation and Response Bias in a Forced-Choice Task,”
Journal of Neurology, Neurosurgery & Psychiatry
55, no. 10 (October 1992): 964–66.
3
. S. Fecteau, A. Pascual-Leone, D. H. Zald, P. Liguori, H. Theoret, P. S. Boggio, and F. Fregni, “Activation of Prefrontal Cortex by Transcranial Direct Current Stimulation Reduces Appetite for Risk During Ambiguous Decision Making,”
Journal of Neuroscience
27, no. 23 (2007): 6212–18.
4
. These results were presented in December 2011 at the Neural Information Processing Systems’ Machine Learning and Interpretation in Neuroimaging workshop in Sierra Nevada, Spain.
5
. R. Verheul, W. van den Brink, and P. Geerlings, “A Three-Pathway Psychological Model of Craving for Alcohol,”
Alcohol and Alcoholism
34 (1999): 197–222.
6
. James Olds and Peter Milner, “Positive Reinforcement Produced by Electrical Stimulation of the Septal Area and Other Regions of Rat Brain,”
Journal of Comparative and Physiological Psychology
47, no. 6 (1954): 419–27.
7
. In 1998, Dr. Lynn Churchill from Washington State University demonstrated that the brain’s connections
actually reorganize
in response to reduced dopamine, resulting in changes in the way opiates affect motor activity. This is just one of many examples of how the brain’s connections adapt and change in response to decreased (and increased) dopamine.
8
. Nassima Ait-Daoud, John D. Roache, Michael A. Dawes, Lei Liu, Xin-Qun Wang, Martin A. Javors, Chamindi Seneviratne, and Bankole A. Johnson, “Can Serotonin Transporter Genotype Predict Craving in Alcoholism?”
Alcoholism: Clinical & Experimental Research
33, no. 8 (2009): 1329–35.
9
. For a nice review of the relationship between serotonin and alcoholism, see David LeMarquanda, Robert O. Pihl, and Chawki Benkelfat, “Serotonin and Alcohol Intake, Abuse, and Dependence: Clinical Evidence,”
Biological Psychiatry
36, no. 5 (1994): 326–37.
10
. P. Huttnen and R. D. Myers, “Anatomical Localization in Hippocampus of Tetrahydro-Beta-Carboline Induced Alcohol Drinking in the Rat,”
Alcohol
4, no. 3 (1987): 181–87.
11
. For a more detailed review of this hypothesis, see K. Blum, E. R. Braverman, J. M. Holder, J. F. Lubar, V. J. Monastra, D. Miller, J. O. Lubar, T. J. Chen, and D. E. Comings, “Reward Deficiency Syndrome: A Biogenetic Model for the Diagnosis and Treatment of Impulsive, Addictive, and Compulsive Behaviors,”
Journal of Psychoactive Drugs
32, Suppl. i–iv (2000): 1–112.
12
. For a great review of this and other theories, see Giovanni Addolorato, Lorenzo Leggio, Ludovico Abenavoli, Giovanni Gasbarrini on behalf of the Alcoholism Treatment Study Group, “Neurobiochemical and Clinical Aspects of Craving in Alcohol Addiction: A Review,”
Addictive Behaviors
30 (2005): 1209–24.
13
. Alec Horniman is the Killgallon Ohio Art Professor of Business Administration and a Senior Fellow of the Olsson Center for Applied Ethics. He teaches ethics, strategy, and leadership at the Darden Graduate School of Business at the University of Virginia.
14
. Rachel L. Goldman, Jeffrey J. Borckardt, Heather A. Frohman, Patrick M. O’Neil, Alok Madan, Laura K. Campbell, Amanda Budak, and Mark S. George, “Prefrontal Cortex Transcranial Direct Current Stimulation (TDCS) Temporarily Reduces Food Cravings and Increases the Self-Reported Ability to Resist Food in Adults with Frequent Food Craving,”
Appetite
56, no. 3 (2011): 741–46.