Examination Medicine: A Guide to Physician Training (88 page)
Read Examination Medicine: A Guide to Physician Training Online
Authors: Nicholas J. Talley,Simon O’connor
Tags: #Medical, #Internal Medicine, #Diagnosis

Deformity
Muscle wasting
Metacarpophalangeal joints
Skin
Swelling – distribution
Deformity – ulnar deviation, volar subluxation etc.
Proximal and distal interphalangeal joints
Skin
Swelling – distribution
Deformity–swan necking, boutonnière (
Fig 16.58
), Z, sausage-shaped etc.
Nails
Psoriatic changes – pitting, ridging, onycholysis, hyperkeratosis, discolouration
Palmar aspect
Skin – scars, palmar erythema (
Fig 16.55
), palm creases (anaemia), discolouration
Muscle wasting
3.
FEEL AND MOVE PASSIVELY
Wrists
Synovitis
Effusions
Range of movement
Crepitus
Ulnar styloid tenderness
Metacarpophalangeal joints
Synovitis
Effusions
Range of movement
Crepitus
Subluxation
Proximal and distal interphalangeal joints
As above
Palmar tendon crepitus
Carpal tunnel syndrome tests
4.
HAND FUNCTION
Grip strength
Key grip
Opposition strength
Practical ability
5.
OTHER
Elbows – subcutaneous nodules, psoriatic rash
Other joints
Signs of systemic disease
1.
First make the patient comfortable, expose as much of the hands and forearms as possible and place the patient’s hands on a pillow, palms down. You may talk as you go. We believe this is the best way to proceed with a joint examination. However, also practise examining this sort of case by presenting at the end of the examination. Be gentle while examining – do not hurt the patient.
2.
If the patient has arthropathy with an obvious rheumatoid distribution, start by stating that the patient has a symmetrical deforming polyarthropathy involving the wrists and hands. Then describe the forearms and wrists – look at the skin for erythema, ecchymoses or skin atrophy (this may indicate steroid use), scars and rashes (e.g. psoriasis: look over the elbows, in the scalp and around the umbilicus). Look for rheumatoid nodules.
3.
Then look for swelling and its distribution, wrist deformity and muscle wasting involving the forearms and interosseous muscles.
4.
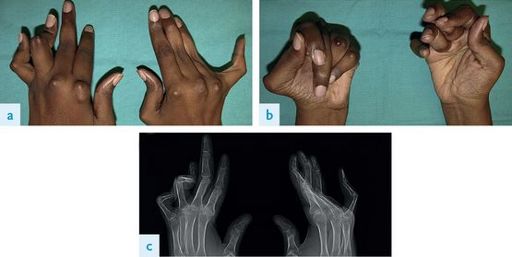
Go on to the metacarpophalangeal (MCP) joints. Mention, if present, any skin abnormalities, swelling and deformity (
Fig 16.56
), particularly ulnar deviation and volar subluxation.

FIGURE 16.56
(a) and (b) Swollen joints in psoriatic arthritis over the second and third metacarpophalangeal joints of the hands. A Garg, D Gladman. Recognizing psoriatic arthritis in the dermatology clinic.
Capsule Summary Journal of the American Academy of Dermatology
, 2010. 63(5):733–748, Figs 3 and 5. American Academy of Dermatology Inc.
5.
Next describe the proximal and distal interphalangeal (PIP and DIP) joints. Symmetrical wrist, MCP and proximal joint swellings suggest rheumatoid arthritis. Swelling in the PIP joints and DIP joints is suggestive of osteoarthritis.
6.
Again mention any skin changes that may be present, swelling over each joint if present and deformity, particularly ‘swan necking’ and boutonnière deformity of the fingers, and ‘Z’ deformity of the thumb. Sausage-shaped phalanges and telescoping of the fingers with predominant interphalangeal joint disease usually means psoriatic arthropathy or Reiter’s disease (see
Fig 16.57
). Small joint ankylosis is common. Look for telangiectasiae.

FIGURE 16.57
Keratoderma blenorrhagicum (Reiter syndrome). The palms and soles are commonly involved. There are keratoic papules, plaques, and pustules that coalesce to form circular borders like those seen on the penis. T P Habif.
Clinical dermatology
, 5th edn. Fig 8.13. Mosby, Elsevier, 2009, with permission.
7.
Next look at the nails and describe any psoriatic nail changes (present in the great majority of patients with psoriatic arthritis) – namely pitting, onycholysis, hyperkeratosis, ridging and discolouration. Note the signs of vasculitis (splinter haemorrhages or black to brown 1–2 mm skin infarcts, usually in a periungual location) and mention this to the examiners.
8.
Now ask the patient to open and close the hands. This will reveal tendon ruptures and fixed flexion deformities.
9.
Turn the wrists over and look at the palms for scars (
Fig 16.55
), palmar erythema and muscle wasting.

FIGURE 16.55
Scars from previous tendon surgery and palmar erythema.
10.
Now go on and palpate each joint, starting with the wrists. Feel for synovitis (boggy swelling) and effusions. Describe the range of passive movement of the joint. Also note any joint crepitus. Palpate the ulnar styloid for tenderness. When examining the MCP joints, also feel for subluxation. Test for palmar tendon crepitus (tenosynovitis).
11.
Having examined each joint, assess the function of the hand. This is very important. Test grip strength, key grip and opposition strength (thumb and little finger), and ask the patient to perform a practical procedure, such as undoing a button.
12.
A formal neurological examination of the hand is not required in assessing arthropathy. However, a ganglion or tenosynovitis may cause the carpal tunnel syndrome. Ask the patient to flex both wrists together for 30 seconds – paraesthesiae will often be precipitated in the affected hand if the carpal tunnel syndrome is present (Phalen’s wrist flexion test). Tap over the carpal tunnel while the wrist is held in extension for Tinel’s sign (paraesthesiae in the distribution of the median nerve). These tests have similar but limited specificity and sensitivity. After you have finished with the hands, feel at the elbows for rheumatoid nodules and look carefully for any psoriatic rash there also.
13.
If function has been mentioned, check sensation in the median and ulna nerve distributions.
You should now have an idea of the pattern and severity of the deformity, as well as the extent of the loss of function and the activity of the disease. Always consider the differential diagnosis of a deforming polyarthropathy:
•
rheumatoid arthritis (see
Figs 16.58
,
16.59
and
16.66
)