Girl, Interrupted (13 page)
Authors: Susanna Kaysen

If the biochemists were able to demonstrate the physical workings of neuroses (phobias, or difficulties getting pleasure from life), if they could pinpoint the chemicals and impulses and interbrain conversations and information exchanges that constitute these feelings, would the psychoanalysts pack up their ids and egos and retire from the field?
They have partially retired from the field. Depression, manic-depression, schizophrenia: All that stuff they always had trouble treating they now treat chemically. Take two Lithium and don’t call me in the morning because there’s nothing to say; it’s innate.
Some cooperative efforts—the sort the brain makes—would be useful here.
For nearly a century the psychoanalysts have been writing op-ed pieces about the workings of a country they’ve never traveled to, a place that, like China, has been off-limits. Suddenly, the country has opened its borders and is crawling with foreign correspondents; neurobiologists are filing ten stories a week, filled with new data. These two groups of writers, however, don’t seem to read each other’s work.
That’s because the analysts are writing about a country they call Mind and the neuroscientists are reporting from a country they call Brain.
Borderline Personality Disorder
*
An essential feature of this disorder is a pervasive pattern of instability of self-image, interpersonal relationships, and mood, beginning in early adulthood and present in a variety of contexts.
A marked and persistent identity disturbance is almost invariably present. This is often pervasive, and is manifested by uncertainty about several life issues, such as self-image, sexual orientation, long-term goals or career choice, types of friends or lovers to have, and which values to adopt. The person often experiences this instability of self-image as chronic feelings of emptiness and boredom.
Interpersonal relationships are usually unstable and intense, and may be characterized by alternation of the extremes of overidealization and devaluation. These people have difficulty tolerating being alone, and will make frantic efforts to avoid real or imagined abandonment.
Affective instability is common. This may be evidenced by marked mood shifts from baseline mood to depression, irritability, or anxiety, usually lasting a few hours or, only rarely, more than a few days. In addition, these people often have inappropriately intense anger with frequent displays of temper or recurrent physical fights. They tend to be impulsive, particularly in activities that are potentially self-damaging, such as shopping sprees, psychoactive substance abuse, reckless driving, casual sex, shoplifting, and binge eating.
Recurrent suicidal threats, gestures, or behavior and other self-mutilating behavior (e.g., wrist-scratching) are common in the more severe forms of the disorder. This behavior may serve to manipulate others, may be a result of intense anger, or may counteract feelings of “numbness” and depersonalization that arise during periods of extreme stress.…
Associated Features
. Frequently this disorder is accompanied by many features of other Personality Disorders, such as Schizotypal, Histrionic, Narcissistic, and Antisocial Personality Disorders. In many cases more than one diagnosis is warranted. Quite often social contrariness and a generally pessimistic outlook are observed. Alternation between dependency and self-assertion is common. During periods of extreme stress, transient psychotic symptoms may occur, but they are generally of insufficient severity or duration to warrant an additional diagnosis.
Impairment
. Often there is considerable interference with social or occupational functioning.
Complications
. Possible complications include Dysthymia [depressive neurosis], Major Depression, Psychoactive Substance Abuse, and psychotic disorders such as Brief Reactive Psychosis. Premature death may result from suicide.
Sex Ratio
. The disorder is more commonly diagnosed in women.
Prevalence
. Borderline Personality Disorder is apparently common.
Predisposing and Familial Pattern
. No information.
Differential Diagnosis
. In Identity Disorder there is a similar clinical picture, but Borderline Personality Disorder preempts the diagnosis of Identity Disorder if the criteria for Borderline Personality Disorder are met, the disturbance is sufficiently pervasive and persistent, and it is unlikely that it will be limited to a developmental stage.…
*
From the
Diagnostic and Statistical Manual of Mental Disorders
, 3d edition, revised (1987), pp. 346–47
My Diagnosis
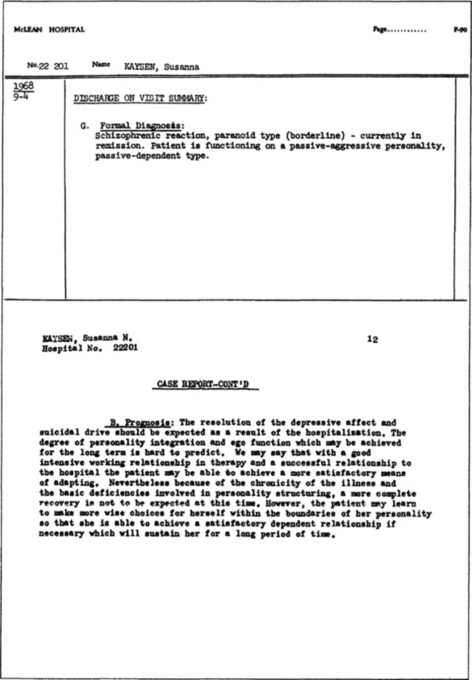
So these were the charges against me. I didn’t read them until twenty-five years later. “A character disorder” is what they’d told me then.
I had to find a lawyer to help me get my records from the hospital; I had to read line 32a of form Al of the Case Record, and entry G on the Discharge on Visit Summary, and entry B of Part IV of the Case Report; then I had to locate a copy of the
Diagnostic and Statistical Manual of Mental Disorders
and look up Borderline Personality to see what they really thought about me.
It’s a fairly accurate picture of me at eighteen, minus a few quirks like reckless driving and eating binges. It’s accurate but it isn’t profound. Of course, it doesn’t aim to be profound. It’s not even a case study. It’s a set of guidelines, a generalization.
I’m tempted to try refuting it, but then I would be open to the further charges of “defensiveness” and “resistance.”
All I can do is give the particulars: an annotated diagnosis.
“[U]ncertainty about several life issues, such as self-image, sexual orientation, long-term goals or career choice, types of friends or lovers to have …” I relish that last phrase. Its awkwardness (the “to have” seems superfluous) gives it substance and heft. I still have that uncertainty. Is this the type of friend or lover I want to have? I ask myself every time I meet someone new. Charming but shallow; good-hearted but a bit conventional; too handsome for his own good; fascinating but probably unreliable; and so forth. I guess I’ve had my share of unreliables. More than my share? How many would constitute more than my share?
Fewer than for somebody else—somebody who’d never been called a borderline personality?
That’s the nub of my problem here.
If my diagnosis had been bipolar illness, for instance, the reaction to me and to this story would be slightly different. That’s a chemical problem, you’d say to yourself, manic-depression, Lithium, all that. I would be blameless, somehow. And what about schizophrenia—that would send a chill up your spine. After all, that’s real insanity. People don’t “recover” from schizophrenia. You’d have to wonder how much of what I’m telling you is true and how much imagined.
I’m simplifying, I know. But these words taint everything. The fact that I was locked up taints everything.
What does
borderline personality
mean, anyhow?
It appears to be a way station between neurosis and psychosis: a fractured but not disassembled psyche. Though to quote my post-Melvin psychiatrist: “It’s what they call people whose lifestyles bother them.”
He can say it because he’s a doctor. If I said it, nobody would believe me.
An analyst I’ve known for years said, “Freud and his circle thought most people were hysterics, then in the fifties it was psychoneurotics, and lately, everyone’s a borderline personality.”
When I went to the corner bookstore to look up my diagnosis in the
Manual
, it occurred to me that I might not find it in there anymore. They do get rid of things—homosexuality, for instance. Until recently, quite a few of my friends would have found themselves documented in that book along with me. Well, they got out of the book and I didn’t. Maybe in another twenty-five years I won’t be in there either.
“[I]nstability of self-image, interpersonal relationships, and mood … uncertainty about … long-term goals or career choice …” Isn’t this a good description of adolescence? Moody, fickle, faddish, insecure: in short, impossible.
“[S]elf-mutilating behavior (e.g., wrist-scratching) …” I’ve skipped forward a bit. This is the one that caught me by surprise as I sat on the floor of the bookstore reading my diagnosis. Wrist-scratching! I thought I’d invented it. Wrist-banging, to be precise.
This is where people stop being able to follow me. This is the sort of stuff you get locked up for. Nobody knew I was doing it, though. I never told anyone, until now.
I had a butterfly chair. In the sixties, everyone in Cambridge had a butterfly chair. The metal edge of its upturned seat was perfectly placed for wrist-banging. I had tried breaking ashtrays and walking on the shards, but I didn’t have the nerve to tread firmly. Wrist-banging—slow, steady, mindless—was a better solution. It was cumulative injury, so each bang was tolerable.
A solution to what? I quote from the
Manual
: “This behavior may … counteract feelings of ‘numbness’ and depersonalization that arise during periods of extreme stress.”
I spent hours in my butterfly chair banging my wrist. I did it in the evenings, like homework. I’d do some homework, then I’d spend half an hour wrist-banging, then finish my homework, then back in the chair for some more banging before brushing my teeth and going to bed. I banged the inside, where the veins converge. It swelled and turned a bit blue, but considering how hard and how much I banged it, the visible damage was slight. That was yet one more recommendation of it to me.
I’d had an earlier period of face-scratching. If my fingernails hadn’t been quite short, I couldn’t have gotten away with it. As it was, I definitely looked puffy and peculiar the next day. I used to scratch my cheeks and then rub soap on them. Maybe the soap prevented me from looking worse. But I looked bad enough that people asked, “Is something wrong with your face?” So I switched to wrist-banging.
I was like an anchorite with a hair shirt. Part of the point was that nobody knew about my suffering. If people knew and admired—or abominated—me, something important would be lost.
I was trying to explain my situation to myself. My situation was that I was in pain and nobody knew it; even I had trouble knowing it. So I told myself, over and over, You are in pain. It was the only way I could get through to myself (“counteract feelings of ‘numbness’ ”). I was demonstrating, externally and irrefutably, an inward condition.
“Quite often social contrariness and a generally pessimistic outlook are observed.” What do you suppose they mean by “social contrariness”? Putting my elbows on the table? Refusing to get a job as a dental technician? Disappointing my parents’ hope that I would go to a first-rate university?
They don’t define “social contrariness,” and I can’t define it, so I think it ought to be excluded from the list. I’ll admit to the generally pessimistic outlook. Freud had one too.
I can honestly say that my misery has been transformed into common unhappiness, so by Freud’s definition I have achieved mental health. And my discharge sheet, at line 41, Outcome with Regard to Mental Disorder, reads “Recovered.”
Recovered. Had my personality crossed over that border, whatever and wherever it was, to resume life within the confines of the normal? Had I stopped arguing with my personality and learned to straddle the line between sane and insane? Perhaps I’d actually had an identity disorder. “In Identity Disorder there is a similar clinical picture, but Borderline Personality … preempts the diagnosis … if the disturbance is sufficiently pervasive and … it is unlikely that it will be limited to a developmental stage.” Maybe I was a victim of improper preemption?
I’m not finished with this diagnosis.
“The person often experiences this instability of self-image as chronic feelings of emptiness or boredom.” My chronic feelings of emptiness and boredom came from the fact that I was living a life based on my incapacities, which were numerous. A partial list follows. I could not and did not want to: ski, play tennis, or go to gym class; attend to any subject in school other than English and biology; write papers on any assigned topics (I wrote poems instead of papers for English; I got F’s); plan to go or apply to college; give any reasonable explanation for these refusals.
My self-image was not unstable. I saw myself, quite correctly, as unfit for the educational and social systems.
But my parents and teachers did not share my self-image. Their image of me was unstable, since it was out of kilter with reality and based on their needs and wishes. They did not put much value on my capacities, which were admittedly few, but genuine. I read everything, I wrote constantly, and I had boyfriends by the barrelful.
“Why don’t you do the assigned reading?” they’d ask. “Why don’t you write your papers instead of whatever you’re writing—what is that, a short story?” “Why don’t you expend as much energy on your schoolwork as you do on your boyfriends?”