i bc27f85be50b71b1 (13 page)
Read i bc27f85be50b71b1 Online
Authors: Unknown

stasis of the blood. Patients with a PT greater than 2.5 times the reference range should not undergo physical therapy because of the potential for spontaneous bleeding. Likewise, an international normalized ratio of more than 3 warrants asking the physician if treatment
should be withheldP
Blood Lipids
Elevated total cholesterol levels in the blood are a significant risk
factor for atherosclerosis and therefore ischemic heart disease.29
Measuring blood cholesterol level is necessary ro determine the risk
for development of atherosclerosis and to assist in patient education, dietary modification, and medical management. Normal values can be adjusted for age; however, levels of more than 240 mg/dl are
generally considered high, and levels of less than 200 mg/dl are considered normal.
A blood lipid analysis categorizes cholesterol into high-density
lipoprotiens ( HDLs) and low-density lipoproteins (LDLs) and provides an analysis of triglycerides.
HDLs are formed by the liver and are considered beneficial because
they are readily transportable and do nOt adhere to the intimal walls


CARDIAC SYSTEM
29
of the vascular system. People with higher amounts of HDLs are at
lower risk for coronary artery disease.27,29 HDL levels of less than 33
mg/dl carry an elevated risk of heart disease, and a more important
risk for heart disease is an elevated ratio of total cholesterol to HDL
Normal toral cholesterol to HDL ratios range from 3 to 5."
LDLs are formed by a diet excessive in fat and are related to a
higher incidence of coronary artery disease. Low-densiry lipoproteins
are nOt as readily transportable, because they adhere to intimal walls
in the vascular system .21 Normal LDLs are below 100 mg/dl,"
Triglycerides are fat cells that are free floating in the blood, When
not in use, they are stored in adipose tissue. Their levels increase after
eating foods high in fat and decrease with exercise. High levels of triglycerides are associated with a risk of coronary heart diseaseP
Clinical Tip
Cholesterol levels may be falsely elevated after an acute
MI; therefore, pre-infarction levels (if known) are used to
guide risk factor modification. Values will not return to
normal until at least 6 weeks post-M!.
Biochemical Markers
After an initial myocardial insult, the presence of tissue necrosis can
be determined by increased levels of biochemical markers. Levels of
biochemical markers, such as serum enzymes (creatine kinase [CK),
lactate dehydrogenase [LDHJ) and proteins (myoglobin, troponin I
and T), can also be used to determine the extent of myocardial death
and the effectiveness of reperfusion therapy, In patients presenting
with specific anginal symptoms and diagnostic ECG, these biochemical markers assist with confirmation of the diagnosis of an M I (Table 1-1 1). Enzymes play a more essential role in medical assessment of
the many patients with nonspecific or vague symptoms and inconclusive ECG changes,30 Such analysis also includes evaluation of isoenzyme levels as wel1,31 Isoenzymes are different chemical forms of the same enzyme that are tissue specific and allow differentiation of damaged tissue (e,g" skeletal muscle vs, cardiac muscle), CK (formally called creatille phosphokinase) is released after cell
injury or cell death. CK has three isoenzymes. The CK-MB isoenzyme
is related to cardiac muscle cell injury or death, The most widely used



30 AClITE CARE HANDBOOK FOR PHYSICAL THERAPISTS
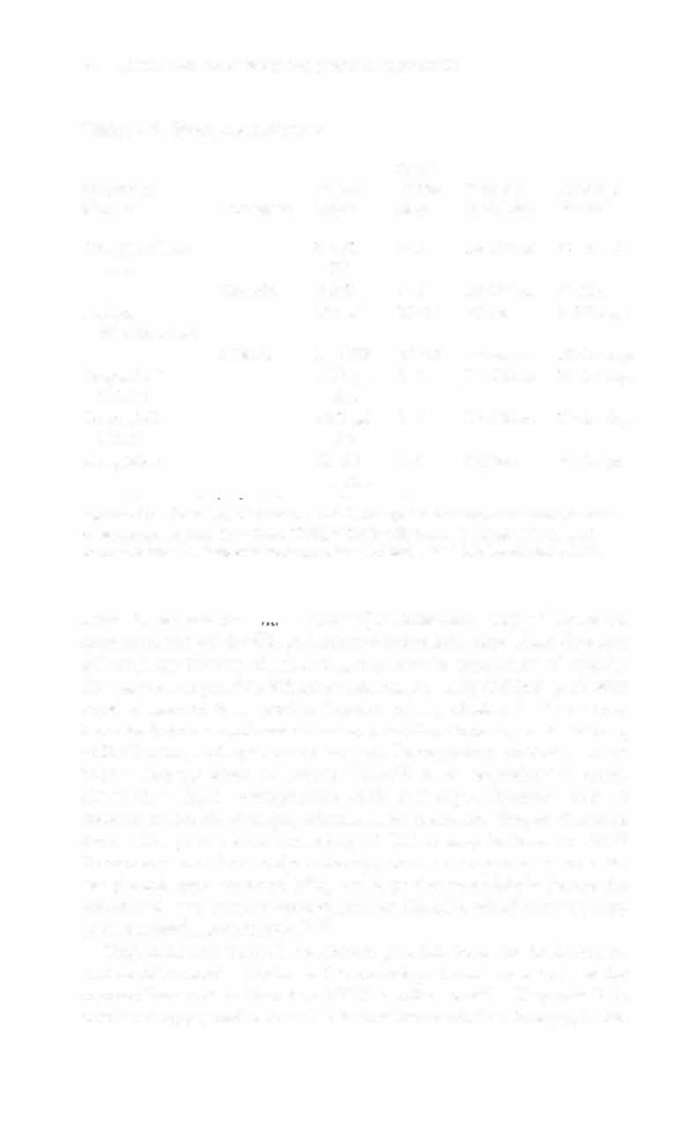
Table 1 - 1 1 . Biochemical Markers
Onset
Enzyme or
Normal
of Rise Time of
Return to
Marker
Isoenzyme
Value
(hrs)
Peak Rise
Normal
Creatine kinase
55-7 1
3-6
1 2-24 hrs 24-48 hrs
(CK)
IU
CK-MB
0-3%
4-8
1 8-24 hrs 72 hrs
Lactate
1 27 1U
1 2-24
72 hrs
5- 1 4 days
dehydrogenase
LDH-I
14-26%
24-72
3-4 days
1 0- 1 4 days
Troponin T
<0.2 �g/
2-4
24-36 hrs
10-14 days
(cTnT)
liter
Troponin I
d . 1 pg/
2-4
24-36 hrs
10- 1 4 days
(cTnl)
liter
Myoglobin
3 1-80
1-2
6-9 hrs
24-36 hrs
ng/ml
Sources: Data from RH Christenson, HME Azzazy. Biochemical markers oC Ihe acute
coronary syndromes. Clin Chern 1 998;44: 1855-1 864; and AK Kratz, KB Leq:md
Rawski. Normal reference laboratory values. N Engl ] Med 1 998;339: 1 063-1072.
value is the relative
( 100%[CK-MBrrotal CKj).30 Temporal
measurements of the CK-MB relative index help physicians diagnose
MI, estimate the size of infarction, evaluate the occurrence of reperfusion as well as possible infarct extension. An early CK-MB peak with rapid clearance is a good indication of reperfusion.'2 Values may
increase from skeletal muscle trauma, cardiopulmonary resuscitation,
defibrillation, and open-heart surgery. Postoperative coronary artery
bypass surgery tends to elevate CK-MB levels secondary to crossclamp time. Early postoperative peaks and rapid clearance seem to indicate reversible damage, whereas la[er peaks and longer clearance
times with peak values exceeding 50 Ulliter may indicate an ML 12
Treatment with thrombolytic therapy, such as streptokinase or a tissue plasminogen activaror (tPa), has been shown to falsely elevate the values and may create a second peak of CK-MB, which strongly suggests successful reperfusion.'2•30
Troponins are essential contractile proteins found in both skeletal