Oxford Handbook of Midwifery (122 page)
Read Oxford Handbook of Midwifery Online
Authors: Janet Medforth,Sue Battersby,Maggie Evans,Beverley Marsh,Angela Walker

- Ensure that the couple considers all the possible different scenarios that may affect their decision, particularly in respect of current children or future relationship breakdown.
- A particular worry in a lot of men is about their ability to maintain erections and have sexual intercourse following vasectomy. Vasectomy does not affect libido or erections, and they will ejaculate normally, but ejaculate will not contain sperm.
- Contraception is required for at least 3 months following vasectomy.
- There is no proven link between vasectomy and the incidence of testicular or prostatic cancer.
- Ensure that the decision that is made is without influence or coercion from healthcare professionals.
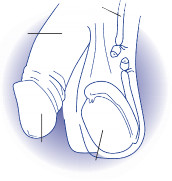
vas deferens
penis

glans
testicle
Fig. 22.9
Male sterilization.Copyright © fpa 2008 and reproduced with permission of the publisher.
CHAPTER 22
Contraception570
Female sterilization
- This is the only permanent form of female contraception.
- Usually a daycare procedure under regional or general anaesthesia.
- Involves incising and dissecting or blocking the fallopian tubes, preventing fertilization (Fig. 22.10).
- It is performed either by laparoscopy, mini-laparotomy, or vaginally.
Efficacy
Highly effective, with an efficacy rate of 99.4–99.8 per 100 woman years.
Disadvantages
- Involves a surgical procedure and anaesthesia.
- Not easily reversed and must be regarded as permanent.
- If it fails, there is a greater risk of ectopic pregnancy.
Advantages
- Permanent.
- Effective immediately.
- The anxiety of unplanned pregnancy is removed.
- The ultimate decision is the woman’s.
 Contraindications
Contraindications - Indecision by either partner (if a partner is involved).
- Relationship problems.
- Psychiatric illness.
- A health problem or disability that may increase the risk of the surgical procedure.
Relative contraindications
- Obesity may be a contraindication for laparoscopy.
- Request for sterilization for a young woman <25.
Counselling prior to sterilization
- This is extremely important, because of the permanency of the method.
- 2 Postoperative regret and grief for lost fertility happens in at least 10% of sterilized women and this must be discussed and the procedure considered thoroughly.
- Whenever possible, discussion should be undertaken with the couple together, to get each partner’s perspective.
Practice points
- When discussing sterilization, it is important to emphasize that sterilization is not normally carried out at the time of termination of pregnancy, vaginal birth, or caesarean section, due to the increased vascularity of the tissue involved. This will increase the failure rate.
- In the UK, sterilization reversal is not carried out on the NHS, except in very exceptional circumstances.
FEMALE STERILIZATION
571
- This is the only permanent form of female contraception.
- Termination of pregnancy or birth is an emotive time and a decision for sterilization made at this time is fraught with potential future psychological and psychosexual problems.
- It is normal to wait at least 6 weeks following termination of pregnancy or birth.
- Unless the mother is fully breastfeeding, effective contraception in the interim period is essential to prevent pregnancy.
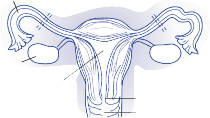
fallopian tube
ovary
uterus

cervix vagina

- (b) (c)
Fig. 22.10
Female sterilization. (a) Tubal ligation; (b) Falope ring; and (c) Filschie clip.Copyright © fpa 2008 and reproduced with permission of the publisher.
CHAPTER 22
Contraception572
Emergency contraception
There are three forms of emergency post-coital contraception:
- The levonorgestrel-only oral preparation, known in the UK as Levonelle
®
, commonly known as the ‘morning after pill’, although this terminology should be discouraged, as it is misleading. - The ulipristal acetate oral preparation, known in the UK as ellaOne
®
,
with increased effectiveness from 72h and up to 5 days post coitally over Levonelle
®
. - A copper IUD.
0 The ‘Mirena
®
’ IUS should not be used for this purpose.How do they work?
- These methods inhibit implantation, should unwanted conception have occurred.
- The primary action of ellaOne
®
is to delay or inhibit ovulation and alter the endometrium, which may also contribute to efficacy. - This must be explained carefully, as personal beliefs about whether life begins at conception or at implantation may affect a woman’s decision about whether to take the emergency contraception pill or to have an IUD inserted.
 Oral pill
Oral pill - The Levonelle
®
tablet is taken within 72h of unprotected sexual intercourse or contraceptive failure to give maximum protection, but it can be taken up to 5 days after intercourse. If taken within 24h, the efficacy rate is 99.6%, and 98.9% at 72h. - The ellaOne
®
tablet is taken orally as soon as possible, but no later than 120h of unprotected sexual intercourse or contraceptive failure. - In explaining the mode of action and efficacy of the emergency contraceptive pill, it is vital to ensure that the woman clearly understands that this relates only to the immediately preceding 72h, even if there are multiple episodes of intercourse within this period.
1 - 0 Any episodes in the current cycle occurring prior to this 72h period may have already resulted in pregnancy and render emergency contraception totally ineffective.
- Treatment with Levonelle
®
, may be repeated in any menstrual cycle, if necessary. However, ellaOne
®
, is not currently recommended to be used more than once per cycle, as the efficacy of repeated exposure has not been assessed. - ellaOne
®
has been shown to be more effective compared to levonorgestrel in women who are categorized as overweight or obese. - There is no evidence of any effect on the fetus, if taken in early pregnancy.
- If there is any doubt about whether pregnancy is possible, carry out a reliable pregnancy test prior to administration. The trophoblast embeds in the uterus in 5–7 days after conception and a reliable
dipstick test, which takes a maximum of 5min, should give the answer.
- It is professionally responsible for the midwife to discuss ongoing reliable methods of contraception with the woman and to give her information or refer her to a contraception and sexual health clinic, or
- The levonorgestrel-only oral preparation, known in the UK as Levonelle
EMERGENCY CONTRACEPTION
573
a doctor trained and currently up to date with contraceptive methods, if hormonal methods are required, or to a midwife or nurse competent in the non-hormonal methods.
Side-effects
- (b) (c)
Other books
It Rained Red Upon the Arena by Kenneth Champion
Florence of Arabia by Christopher Buckley
Die I Will Not by S K Rizzolo
A Long Tall Texan Summer: Tom Walker by Diana Palmer
B006U13W The Flight (Jenny Cooper 4) nodrm by Hall, M. R.
Landing by J Bennett
The Life Engineered by J. F. Dubeau
His Southern Sweetheart by Carolyn Hector
West of January by Dave Duncan
Slain in Schiaparelli (Vintage Clothing Mysteries Book 3) by Angela M. Sanders