Read Pediatric Examination and Board Review Online
Authors: Robert Daum,Jason Canel
Pediatric Examination and Board Review (194 page)

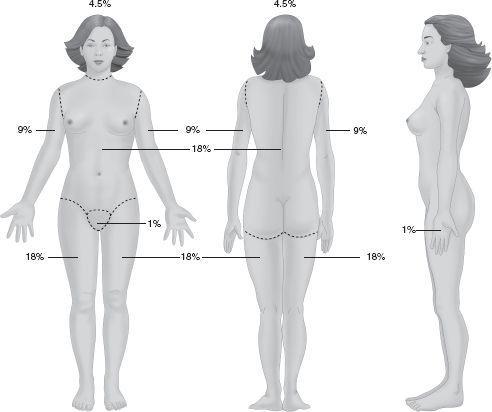
FIGURE 108-2.
The Rule of Nines can be used as a quick reference for estimating a patient’s burn size by dividing the body into regions to which total body surface area is allocated in multiples of nine. (Reproduced, with permission, from Brunicardi FC, Andersen DK, Billiar TR, et al. Schwartz’s Principles of Surgery, 9th ed. New York: McGraw-Hill; 2010: Fig. 8-1.)
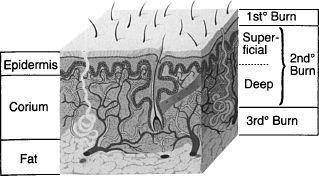
FIGURE 108-3.
Layers of skin showing depth of first-degree, second-degree, and third-degree burns. (Reproduced, with permission, from Doherty G. Current Diagnosis & Treatment: Surgery, 13th ed. New York: McGraw-Hill; 2010: Fig. 14-1.)
5.
(E)
Because this child is 2 years old and tetanus immunization is required if there has not been immunization in the last 5 years, providing local wound care until the immunization status can be ascertained is the correct answer. An unimmunized child requires tetanus immune globulin. Empirical treatment for streptococcal infection is no longer warranted because of the routine use of topical antibiotics in burn care.
6.
(B)
The child in this scenario sustained a scald burn in a stocking distribution, which could be consistent with either an intentional or unintentional immersion. By contacting the child welfare system, the medical provider can assist investigational agents by educating them on burn injuries and by providing crucial historical data that can either be corroborated or refuted to address the truthfulness of the history provided.
7.
(E)
At this point, a skeletal survey would be the best choice. With regard to the evaluation for suspected child abuse, your examination can guide you to necessary tests. On examination this child is alert and well nourished. Her mental status is normal, so you can assess for other traumatic injuries clinically (eg, evidence for acute brain injury or acute abdominal trauma). If, while obtaining prior medical information, there is concern for an old intracranial injury (eg, a change in head circumference), one should obtain imaging of the central nervous system with either a head CT or an MRI. If the child starts to show symptoms such as vomiting, a workup for an occult CNS or GI injury can be considered. At this point a skeletal survey alone would be the best choice.
8.
(C)
Epidemiologically speaking, related caretakers are more likely to abuse children than unrelated caretakers.
9.
(E)
The most common type of inflicted burn injuries are scald burns.
10.
(E)
Although they may not affect as much surface area, electrical burn injuries are more extensive than what can be visualized. The injuries are often internal and depend on the voltage and pathway of the electrical current. Myoglobinuria and renal failure can be anticipated with major electrical injuries, and management should include monitoring for cardiac arrhythmias.
11.
(E)
Prior involvement of the caretaker with the child welfare system may impact the disposition of the case, but it does not prove or disprove whether a specific injury was inflicted. Distinguishing between an inflicted and noninflicted injury should be based on the consistency of the history provided with the sustained injury. A collaborative and comprehensive multidisciplinary approach among child welfare, police, and medical staff with training and expertise in child abuse assessment is necessary to increase the likelihood of a correct decision.
12.
(D)
All of the characteristics are important to consider; depth of the bruise is not a characteristic that can be assessed on examination. The age of the patient is important because young infants with bruises should lead the doctor to inquire and ensure the bruises are adequately explained because truly accidental bruising is rarely found in infants.
13.
(B)
Assessing the age of a bruise is a very imprecise process. Many factors affect the rate of healing and resulting color changes, and bruises in the same person that are of identical age and mechanism may not appear the same on examination. One study indicated that yellow discoloration implies at least 18 hours of healing, but it must be emphasized that assessing aging of bruising is very imprecise. A physician can, however, comment on patterns, location, and, in some circumstances, varying ages between healed bruises or between old lesions and new ones.
14.
(C)
These lesions are most likely Mongolian spots or birthmarks because the mother states that the child has had them since birth. Bruising is transient and will heal, so reexamination at a later time will elucidate the diagnosis. Mongolian birthmarks are most often seen in Asian and African American children and disappear by 4 years of age.
15.
(D)
Saline swabs should be obtained from a fresh bite to perform forensic analysis, not to ascertain the flora of the perpetrator’s mouth. The adult bite pattern is different than that of a child’s in that the adult bite will usually only show one arch, and it will only contain dentition marks between the canine teeth. Children’s bite marks often exhibit both arches and include the molars. Photo documentation including a ruler for measurement is invaluable for forensic investigation.
16.
(B)
All of the other answers define MSBP, first described by Sir Roy Meadow in 1977.
17.
(C)
The perpetrators in MSBP rarely confess on their own volition.
18.
(
B
) The ultimate goal of foster care is family reunification.
 S
S
UGGESTED
R
EADING
Fleisher GR, Ludwig S, Henretig BK, eds.
Pediatric Emergency Medicine
. 5th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2005.
Reece RM, Christian CW, eds.
Child Abuse
:
Medical Diagnosis and Management
. 3rd ed. Elk Grove Village, IL: American Academy of Pediatrics; 2009.
CASE 109: AN 8-MONTH-OLD WITH IRRITABILITY
A colleague contacts you requesting advice regarding her 8-month-old girl who has been very fussy for 2 days. The child has been sleepier, irritable, intermittently vomiting, and less consolable than usual. She has had no fever although frequently has felt warm to touch. Your colleague also thought she saw some tremors on one occasion. The pediatrician diagnosed a viral infection and instructed her to encourage fluids and use an antipyretic as necessary. You ultimately agree to evaluate your colleague’s child.
During your assessment you find out that the girl is a first-born child, a product of a 36-week gestation, born by vaginal delivery without complications. The child is breast-fed; mother does pump breast milk so that her daytime caretaker can provide breast milk exclusively. The child has grown well, and developmentally there have been no concerns to date.
On examination, her vital signs are normal and stable; she appears mildly dehydrated and has no fever. She is sleepy but arousable; her eyes remain closed. She seems to be more irritable with holding, and her fontanel appears full but not tense. Her pupils are equal and reactive, tone appears symmetric, no murmurs are appreciated, lung fields are clear, abdomen is soft without any masses, and her skin has no lesions. You advise your colleague that a sepsis evaluation is warranted. The spinal tap yields bloody fluid on 2 attempts. The white count is 7600/mm
3
, the hemoglobin is 9.5 g/dL, and the hematocrit is 29.6%. A urinalysis, blood electrolytes, and glucose measurements are normal. You elect to admit the patient for observation and empirically treat for meningitis.
SELECT THE ONE BEST ANSWER
1.
Based on this child’s history and examination, all of the following tests are indicated except
(A) head CT
(B) abdominal ultrasound
(C) skeletal survey
(D) toxicology screen
(E) electroencephalograph (EEG)
2.
You are concerned this child may have been abused; you attempt a funduscopic examination, but the child is uncooperative. Which of the following statements is true?
(A) the lack of retinal hemorrhages on examination rules out the diagnosis of inflicted head trauma
(B) retinal hemorrhage due to abuse always involves both eyes
(C) examination by an ophthalmologist is indicated
(D) a neurologically intact child will not have retinal hemorrhages
