Pediatric Primary Care Case Studies (36 page)
Read Pediatric Primary Care Case Studies Online
Authors: Catherine E. Burns,Beth Richardson,Cpnp Rn Dns Beth Richardson,Margaret Brady
Tags: #Medical, #Health Care Delivery, #Nursing, #Pediatric & Neonatal, #Pediatrics

What is the prognosis for encopresis?

Even with aggressive medical and behavioral interventions, as many as 30% of children remain symptomatic (Rockney, McQuade, Days, Linn, & Alario, 1996). Consultation with a pediatric gastroenterologist is warranted when therapy fails, when an organic disease is of concern, or when management is complex.
Key Points from the Case
1. Assessment and management of pediatric encopresis is a challenging problem faced by the primary care provider.
2. Because approximately 80–95% of children with encopresis have a history of constipation or painful bowel movements, management usually focuses on disimpaction of stool followed by daily stool softeners to ensure passage of stool without pain.
3.
In addition to stool softeners as the mainstay of treatment, behavioral strategies to promote effective toileting routines are recommended.
4. Progress towards the goal of resolution of soiling is typically slow and tedious. Frequent follow-up by the primary care provider that focuses on continued education about medication dosages, toileting routines and strategies that promote rectal relaxation, age-appropriate rewards and consequences, and importance of consistency is paramount.
5. If therapy fails, consider the adequacy of the disimpaction efforts, compliance of medical management, length of maintenance therapy, and psychosocial issues that may thwart progress. Refer or consult as needed with a pediatric gastroenterologist and/or mental health provider.
REFERENCES
Baker, S., Liptak, G., Colletti, R., Croffie, J., Di Lorenzo, C., Ector, W., & Nurko, S. (2006). Clinical practice guideline: Evaluation and treatment of constipation in infants and children: Recommendations of the North American Society for Pediatric Gastroenterology, Hepatology and Nutrition.
Journal of Pediatric Gastroenterology and Nutrition, 43
, e1–e13.
Borowitz, S. (2008).
Encopresis
. Retrieved May 2008, from
http://www.emedicine.com/ped/TOPIC670.HTM#section~AuthorsandEditors
Castiglia, P. (2001). Constipation in children.
Journal of Pediatric Health Care, 15
(4), 200–202.
Coughlin, E. (2003). Assessment and management of pediatric constipation in primary care.
Pediatric Nursing, 29
(4), 296–301.
Di Lorenzo, C., & Benninga, M. (2004). Pathophysiology of pediatric fecal incontinence.
Gastroenterology, 126(1
Suppl 1), S33–S40.
Gandy, E., Michaia, S., Preud’Homme, D., & Mezoff, A. (2004). PEG for constipation in children younger than eighteen months old.
Journal of Pediatric Gastroenterology and Nutrition, 39
(2), 197–199.
Hyman, P. E., Milla, P. J., Benninga, M. A., et al. (2006). Childhood functional gastrointestinal disorders: Neonate/toddler.
Gastroenterology, 130
, 1519.
Joinson, C., Heron, J., Butler, R., Von Gontard, A., Butler, U., Emond, A., et al. (2007). A United Kingdom population-based study of intellectual capacities in children with and without soiling, daytime wetting, and bed-wetting.
Pediatrics, 120
(2), e308–e316.
Levy, J. (2001).
A guide to children’s digestive and nutritional needs
. Retrieved May 2008, from
http://www.naspghan.org/wmspage.cfm?parm1=104
Loening-Baucke, V., Krishna, R., & Pashankar, D. (2004). PEG 3350 without electrolytes for the treatment of functional constipation in infants and toddlers.
Journal of Pediatric Gastroenterology and Nutrition, 39
(5), 536–539.
Mellon, M., Whiteside, S., & Friedrich, W. (2006). The relevance of fecal soiling as an indicator of child sexual abuse: A preliminary analysis.
Journal of Developmental and Behavioral Pediatrics, 27
(1), 25–32.
Partin, J. C., Hamill, S., Fischel, J. E., & Partin, J. S. (1992). Painful defecation and fecal soiling in children.
Pediatrics, 89
(6 Pt 1), 1007–1009.
Pashankar, D., Lowning-Baucke, V., & Bishop, W. (2003). Safety of PEG 3350 for the treatment of chronic constipation in children with dysfunctional elimination.
Archives of Pediatric and Adolescent Medicine, 157
, 661–664.
Pyles, C., & Gray, J. (1997). Encopresis: An algorithmic approach.
Physician Assistant, 21
(7), 56, 58, 60–62, 67–68, 70–74.
Rasquin, A., Di Lorenzo, C., Fobes, D., et al. (2006). Childhood functional disorders: Child/adolescent.
Gastroenterology, 130
(5):1527–1537.
Rockney, R., McQuade, W., Days, A., Linn, M., & Alario, A. (1996). Encopresis treatment outcome: Long-term follow-up of 45 cases.
Journal of Developmental and Behavioral Pediatrics, 17
(6), 380–385.
Rosen, C., Buonomo, C., Andrade, R., & Nurko, S. (2004). Incidence of spinal cord lesions in patients with intractable constipation.
Journal of Pediatrics, 143
, 409–411.
Thompson, J. (2001). The management of chronic constipation in children.
Community Practitioner, 74
(1), 29–30.
Tobias, N., Mason, D., & Lutkenhoff, M. (2008). Management principles of organic causes of childhood constipation.
Journal of Pediatric Health Care, 22
(1), 12–23. Retrieved June 2008, from
http://www.medscape.com/viewarticle/569470
Youssef, N., Peters, J., Henderson, W., Shultz-Peters, S., Lockhart, D., & Di Lorenzo, C. (2002). Dose response of PEG 3350 for the treatment of childhood fecal impaction.
Journal of Pediatrics, 14
(3), 410–414.
Chapter 10
The Teen Needing a Sports Physical
Catherine G. Blosser
The preparticipation sports examination (PPE) is often the only health examination for the majority of youth and adolescents in any given year. One percent to 8% of teens undergoing a PPE will have findings that require further evaluation or referral prior to authorizing sports participation; fewer than 1% will need to be excluded from sports because of a significant finding (Landry & Logan, 2007). The PPE should be performed according to customary and standard practices; all history and physical findings need to be documented, including any perceived risk factors and advice about potential dangers of participation that have been discussed with the youth and his or her family. (A signed consent is warranted in such a case.) Ideally, the PPE is performed by the primary care provider. Massive sports examination screenings (i.e., examination stations) are offered in many communities to allay costs and time for both the youth and parent. However, there is a loss of continuity from the history to the examination and then to follow-up, a lack of privacy and patient–provider familiarity, and little time for health promotion discussions when this process is used.
Educational Objectives
1. Identify the two parts of the PPE.
2. Apply customary and standard practices for performing a PPE, including a thorough assessment of health status, fitness level, maturity level, and detection of injuries and illnesses that might limit participation and/or lead to morbidity or mortality.
3. Discuss the advantages to using a PPE form.
4. Discuss necessary documentation components of the cardiovascular examination.
5. Discuss lifestyle risk factors and ways to promote healthy choices.
6. Discuss risk factors specific to females athletes.
7. Recommend ways to improve athletic performance.
8. Discuss the pros and cons of mass screenings designed with stations for conducting the PPE that are standard within some school districts.
9. Identify opportunities within your practice community for establishing stronger ties with coaches and trainers.
Case Presentation and Discussion
Nikola Avery is a 16-year-old Caucasian female who is planning to try out for the crosscountry running team at her high school. She comes today with her 20-year-old sister, who is in the waiting room because their parents both work. Nikola has just transferred into the school district from another state; she relates that this will be her second year of running competitively in high school.
You tell Nikola that before doing the physical examination, you want to review the history form she and her mother completed (it is cosigned). This form was sent out by the clinic to the family at the time the appointment was made.
Assessing Risk Factors for Sports Participation
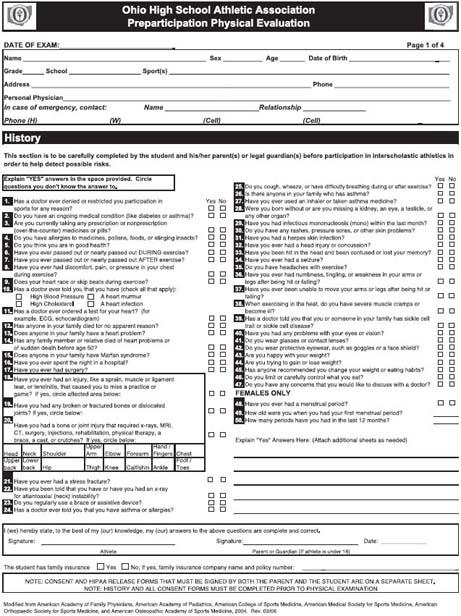
The assessment of a young person for sports participation needs to include any history or physical findings that would alert the provider about the need for further inquiry or raise concerns regarding the activity appropriate for that particular person. A well-designed preparticipation physical examination form would serve this purpose and also allow for a time-efficient examination. A sample form is available in
Figure 10-1
.
What risk factors for sports participation come to your mind?
Risk factors
Risk factors of note include:
• Previous trauma, especially to the musculoskeletal or central nervous system
• Cardiovascular disease (including congenital heart disease, carditis, dysrhythmia, mitral valve prolapse, hypertension above the 90th percentile, and exertional syncope)
• Prior history of heat intolerance
• Chronic medical conditions, including allergic reactions, respiratory problems, sickle cell disease, diabetes, human immunodeficiency virus (HIV), eating disorders, cerebral palsy, and hemophilia
• Seizures
• Infectious mononucleosis
• Skin infections
• Anatomic abnormalities, including missing paired organs, or Down or Marfan syndromes (or history of Marfan syndrome in family)
• Obesity
• In females, menstrual and eating habit irregularities
• Family history of sudden death
Table 10-1
will help the provider determine whether sports participation should be allowed, whether further evaluation is needed before being allowed, or if the risk factor precludes participation. In some cases, an alternative sport can be proposed that reduces risk and allows participation for the individual.