Phantoms in the Brain: Probing the Mysteries of the Human Mind (5 page)
Read Phantoms in the Brain: Probing the Mysteries of the Human Mind Online
Authors: V. S. Ramachandran,Sandra Blakeslee
Tags: #Medical, #Neurology, #Neuroscience

"brakes"—inhibitory messages sent across the corpus callosum from the more rational left hemisphere. But if she had suffered, as Goldstein surmised, damage to the corpus callosum as the result of a stroke, that inhibition would be removed. The right side of her brain and its murderous left hand were now free to attempt to strangle her.
15
This explanation is not as far−fetched as it seems, since it's been well known for some time that the right hemisphere tends to be more emotionally volatile than the left. Patients who have a stroke in the left brain are often anxious, depressed or worried about their prospects for recovery. The reason seems to be that with the left brain injured, their right brain takes over and frets about everything. In contrast, people who suffer damage to the right hemisphere tend to be blissfully indifferent to their own predicament. The left hemisphere just doesn't get all that upset. (More on this in Chapter 7.)
When Goldstein arrived at his diagnosis, it must have seemed like science fiction. But not long after that office visit, the woman died suddenly, probably from a second stroke (no, not from strangling herself). An autopsy confirmed Goldstein's suspicions: Prior to her Strangelovean behavior, she had suffered a massive stroke in her corpus callosum, so that the left side of her brain could not "talk to" nor exert its usual control over the right side. Goldstein had unmasked the dual nature of brain function, showing that the two hemispheres are indeed specialized for different tasks.
Consider next the simple act of smiling, something we all do every day in social situations. You see a good friend and you grin. But what happens when that friend aims a camera at your face and asks you to smile on command? Instead of a natural expression, you produce a hideous grimace. Paradoxically, an act that you perform effortlessly dozens of times each day becomes extraordinarily difficult to perform when someone simply asks you to do it. You might think it's because of embarrassment. But that can't be the answer because if you walk over to any mirror and try smiling, I assure you that the same grimace will appear.
The reason these two kinds of smiles differ is that different brain regions handle them, and only one of them contains a specialized "smile circuit." A spontaneous smile is produced by the basal ganglia, clusters of cells found between the brain's higher cortex (where thinking and planning take place) and the evolutionarily older thalamus. When you encounter a friendly face, the visual message from that face eventually reaches the brain's emotional center or limbic system and is subsequently relayed to the basal ganglia, which orchestrate the sequences of facial muscle activity needed for producing a natural smile. When this circuit is activated, your smile is genuine. The entire cascade of events, once set in motion, happens in a fraction of a second without the thinking parts of your cortex ever being involved.
But what happens when someone asks you to smile while taking your photograph? The verbal instruction from the photographer is received and understood by the higher thinking centers in the brain, including the auditory cortex and language centers. From there it is relayed to the motor cortex in the front of the brain, which specializes in producing voluntary skilled movements, like playing a piano or combing your hair.
Despite its apparent simplicity, smiling involves the careful orchestration of dozens of tiny muscles in the appropriate sequence. As far as the motor cortex (which is not specialized for generating natural smiles) is concerned, this is as complex a feat as playing Rachmaninoff though it never had lessons, and therefore it fails utterly. Your smile is forced, tight, unnatural.
Evidence for two different "smile circuits" comes from brain−damaged patients. When a person suffers a stroke in the right motor cortex—the specialized brain region that helps orchestrate complex movements on the left side of the body—problems crop up on the left. Asked to smile, the patient produces that forced, unnatural grin, but now it's even more hideous; it's a half smile on the right side of the face alone. But when this same patient sees a beloved friend or relative walk through the door, her face erupts into a broad, natural smile using both sides of the mouth and face. The reason is that her basal ganglia have not been damaged by the stroke, so the special circuit for making symmetrical smiles is intact.8
Very rarely, one encounters a patient who has apparently had a small stroke, which neither he nor anyone else notices until he tries to smile. All of a sudden, his loved ones are astonished to see that only one half of his face is grinning. And yet when the neurologist instructs him to smile, he produces a symmetrical, albeit unnatural grin—the exact converse of the previous patient. This fellow, it turns out, had a tiny stroke that only 16
affected his basal ganglia selectively on one side of the brain.
Yawning provides further proof for specialized circuitry. As noted, many stroke victims are paralyzed on the right or left side of their bodies, depending on where the brain injury occurs. Voluntary movements on the opposite side are permanently gone. And yet when such a patient yawns, he stretches out both arms spontaneously. Much to his amazement, his paralyzed arm suddenly springs to life! It does so because a different brain pathway controls the arm movement during the yawn— a pathway closely linked to the respiratory centers in the brain stem.
Sometimes a tiny brain lesion—damage to a mere speck of cells among billions—can produce far−reaching problems that seem grossly out of proportion to the size of the injury. For example, you may think that memory involves the entire brain. When I say the word "rose," it evokes all sorts of associations: perhaps images of a rose garden, the first time someone ever gave you a rose, the smell, the softness of petals, a person named Rose and so on. Even the simple concept of "rose" has many rich associations, suggesting that the whole brain must surely be involved in laying down every memory trace.
But the unfortunate story of a patient known as H.M. suggests otherwise.9 Because H.M. suffered from a particularly intractable form of epilepsy, his doctors decided to remove "sick" tissue from both sides of his brain, including two tiny seahorse−shaped structures (one on each side) called the hippocampus, a structure that controls the laying down of new memories. We only know this because after the surgery, H.M. could no longer form new memories, yet he could recall everything that happened before the operation. Doctors now treat the hippocampus with greater respect and would never knowingly remove it from both sides of the brain (Figure 1.3).
Although I have never worked directly with H.M., I have often seen patients with similar forms of amnesia resulting from chronic alcoholism or hypoxia (oxygen starvation in the brain following surgery). Talking to them is an uncanny experience. For example, when I greet the patient, he seems intelligent and articulate, talks normally and may even discuss philosophy with me. If I ask him to add or subtract, he can do so without trouble. He's not emotionally or psychologically disturbed and can discuss his family and their various activities with ease.
Then I excuse myself to go to the restroom. When I come back, there is not a glimmer of recognition, no hint that he's ever seen me before in his life.
"Do you remember who I am?"
"No."
I show him a pen. "What is this?"
"A fountain pen."
"What color is it?"
"It's red."
I put the pen under a pillow on a nearby chair and ask him, "What did I just do?"
He answers promptly, "You put the pen under that pillow."
17
Then I chat some more, perhaps asking about his family. One minute goes by and I ask, "I just showed you something. Do you remember what it was?"
He looks puzzled. "No."
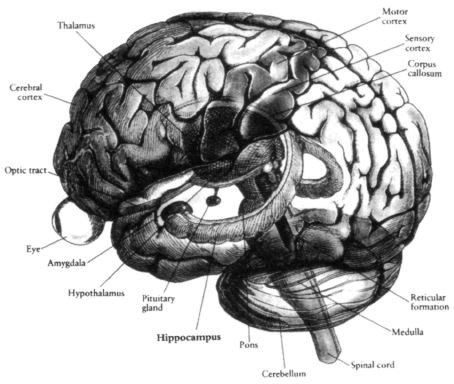
Figure 1.3
Artist's rendering of a brain with the outer convoluted cortex rendered partially transparent to
allow inner structures to be seen. The thalamus (dark) can be seen in the middle, and interposed between it
and the cortex are clusters of cells called the basal ganglia (not shown). Embedded in the front part of the
temporal lobe you can see the dark, almond−shaped amygdala, the "gateway" to the limbic system. In the
temporal lobe you can also see the hippocampus (concerned with memory). In addition to the amygdala, other
parts of the limbic system such as the hypothalamus (below the thalamus) can be seen. The limbic pathways
mediate emotional arousal. The hemispheres are attached to the spinal cord by the brain stem (consisting of
medulla, pons and midbrain), and below the occipital lobes is the cerebellum, concerned mainly with
coordination of movements and timing.
From
Brain, Mind and Behavior
by Bloom and Laserson (1988) by Educational Broadcasting Corporation. Used with permission from W. H. Freeman and Company.
"Do you remember that I showed you an object? Do you remember where I put it?"
"No." He has absolutely no recollection of my hiding the pen sixty seconds earlier.
Such patients are, in effect, frozen in time in the sense they remember only events that took place before the accident that injured them neu−rologically. They may recall their first baseball game, first date and college graduation in elaborate detail, but nothing after the injury seems to be recorded. For example, if post accident they come upon last week's newspaper, they read it every day as if it were a brand−new paper each time. They can read a detective novel again and again, each time enjoying the plot and the surprise ending. I can tell them the same joke half a dozen times and each time I come to the punch line, they laugh heartily (actually, my graduate students do this too).
18
These patients are telling us something very important—that a tiny brain structure called the hippocampus is absolutely vital for laying down new memory traces in the brain (even though the actual memory traces are not stored in the hippocampus). They illustrate the power of the modular approach: In helping to narrow the scope of inquiry, if you want to understand memory, look at the hippocampus. And yet, as we shall see, studying the hippocampus alone will never explain all aspects of memory. To understand how memories are retrieved at a moment's notice, how they are edited, pigeonholed (sometimes even censored!), we need to look at how the hippocampus interacts with other brain structures such as the frontal lobes, the limbic system (concerned with emotions) and the structures in the brain stem (which allow you to attend selectively to specific memories).
The role of the hippocampus in forming memories is clearly established, but are there brain regions specialized in more esoteric abilities like the "number sense" that is unique to humans? Not long ago I met a gentleman, Bill Marshall, who had suffered a stroke a week earlier. Cheerful and on his way to recovery, he was only too happy to discuss his life and medical condition. When I asked him to tell me about his family, he named each of his children, listed their occupations and gave many details about his grandchildren. He was fluent, intelligent and articulate—and not everyone is so soon after a stroke.
"What was your occupation?" I asked Bill.
Bill replied, "I used to be an Air Force pilot."
"What kind of plane did you fly?"
He named the plane and said, "It was the fastest man−made thing on this planet at that time." Then he told me how fast it flew and said that it had been made before the introduction of jet engines.
At one point I said, "Okay, Bill, can you subtract seven from one hundred? What's one hundred minus seven?"
He said, "Oh. One hundred minus seven?"
"Yeah."
"Hmmm, one hundred minus seven."
"Yes, one hundred minus seven."
"So," said Bill. "One hundred. You want me to take away seven from one hundred. One hundred minus seven."
"Yes."
"Ninety six?"
"No."
"Oh," he said.
"Let's try something else. What's seventeen minus three?"
"Seventeen minus three? You know I'm not very good at this kind of thing," said Bill.
19
"Bill," I said, "is the answer going to be a smaller number or a bigger number?"
"Oh, a smaller number," he said, showing that he knew what subtraction is.
"Okay, so what's seventeen minus three?"
"Is it twelve?" he said at last.
I started wondering whether Bill had a problem understanding what a number is or the nature of numbers.
Indeed, the question of numbers is old and deep, going back to Pythagoras.
I asked him, "What is infinity?"
"Oh, that's the largest number there is."
"Which number is bigger: one hundred and one or ninety−seven?
He answered immediately: "One hundred and one is larger."
"Why?"
"Because there are more digits."
This meant that Bill still understood, at least tacitly, sophisticated numerical concepts like place value. Also, even though he couldn't subtract three from seventeen, his answer wasn't completely absurd. He said "twelve,"
not seventy−five or two hundred, implying that he was still capable of making ballpark estimates.