Ross & Wilson Anatomy and Physiology in Health and Illness (121 page)
Read Ross & Wilson Anatomy and Physiology in Health and Illness Online
Authors: Anne Waugh,Allison Grant
Tags: #Medical, #Nursing, #General, #Anatomy

•
The disease may spread:
–
throughout the lung, forming multiple small foci; to the respiratory passages, causing bronchopneumonia or bronchiectasis; to the pleura, with or without effusion
–
to other parts of the body via lymph and blood leading to widespread infection and the development of numerous small foci throughout the body (
miliary tuberculosis
).
Weight loss and malaise develop insidiously, and night sweats are common. Chronic cough, with or without blood in the sputum (haemoptysis) may be present.
Secondary (postprimary) tuberculosis
This occurs only in people carrying a primary lesion, usually in the apex of one or both lungs. It may be caused by a new infection or by reactivation of infection by microbes surviving within Ghon foci, often following reduction of immunity by age or illness. As sensitisation has already occurred, T-lymphocytes stimulate an immediate immune reaction. The subsequent course of the disease is variable. The infection may remain localised in the lung, with complete healing or persistence of live bacteria with their sealed pockets of infection. Progressive destruction of lung tissue leads to cavitation, pleurisy, pleural effusions and empyema (pus in the pleural space). Blood-borne spread may lead to infection of other tissues, e.g. bone and brain. Widely disseminated TB is always fatal unless effectively treated.
Lung tumours

Learning objectives
After studying this section, you should be able to:
describe the pathology of the common lung tumours.
Benign tumours of the lung are rare.
Bronchial carcinoma
Primary bronchial carcinoma is a very common malignancy. The vast majority (up to 90%) of cases occur in smokers or those who inhale other people’s smoke (passive smokers). Other risk factors include exposure to airborne dusts and the presence of lung fibrosis. Very frequently, a metastatic tumour elsewhere causes symptoms before the primary in the lung has been discovered, and therefore the prognosis of this type of cancer is usually poor.
The tumour usually develops in a main bronchus, forming a large friable mass which projects into the lumen, sometimes causing obstruction. Mucus then collects and predisposes to development of infection. As the tumour grows it may erode a blood vessel, causing haemoptysis.
Spread of bronchial carcinoma
This does not follow any particular pattern or sequence. Spread is by infiltration of local tissues and the transport of tumour fragments in blood and lymph. If blood or lymph vessels are eroded, fragments may spread while the tumour is quite small. A metastatic tumour may, therefore, cause symptoms before the primary in the lung has been detected.
Local spread
This may be within the lung, to the other lung or to mediastinal structures, e.g. blood vessels, nerves, oesophagus.
Lymphatic spread
Tumour fragments spread along lymph vessels to successive lymph nodes in which they may cause metastatic tumours. Fragments may enter lymph draining from a tumour or gain access to a larger vessel if its walls have been eroded by a growing tumour.
Blood spread
Tumour cells can enter the blood if a blood vessel is eroded by a growing tumour. The most common sites of blood-borne metastases are the liver, brain, adrenal glands, bones and kidneys.
Pleural mesothelioma
The majority of cases of this malignant tumour of the pleura are linked with previous exposure to asbestos dust, e.g. asbestos workers and people living near asbestos mines and factories. Smoking multiplies the risk of mesothelioma development several fold in people exposed to asbestos. Mesothelioma may develop after widely varying duration of asbestos exposure, from 3 months to 60 years, and is usually associated with crocidolite fibres (blue asbestos). The tumour involves both layers of pleura and as it grows it obliterates the pleural cavity, compressing the lung. Lymph and blood-spread metastases are commonly found in the hilar and mesenteric lymph nodes, the other lung, liver, thyroid and adrenal glands, bone, skeletal muscle and the brain.
Lung collapse (
Fig. 10.31
)
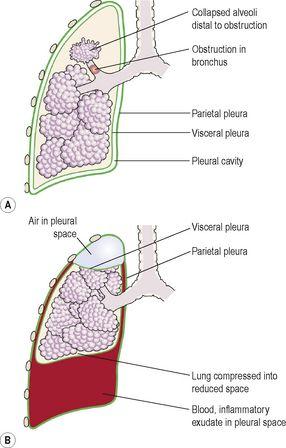
Figure 10.31
Collapse of a lung. A.
Absorption collapse.
B.
Pressure collapse.
Learning objectives
After studying this section, you should be able to:
The clinical effects of collapse of all or part of a lung depend on how much of the lung is affected. Fairly large sections of a single lung can be out of action without obvious symptoms. The term
atelectasis
means lung collapse. There are four main causes of this condition:
•
obstruction of an airway (absorption collapse)
•
impaired surfactant function
•
pressure collapse
•
alveolar hypoventilation.
Obstruction of an airway (absorption collapse,
Fig. 10.31A
)
The amount of lung affected depends on the size of the obstructed air passage. Distal to the obstruction air is trapped and absorbed, the lung collapses and secretions collect. These may become infected, causing abscess formation. Short-term obstruction is usually followed by reinflation of the lung without lasting ill-effects. Prolonged obstruction leads to progressive fibrosis and permanent collapse. Sudden obstruction may be due to inhalation of a foreign body or a mucus plug formed during an asthmatic attack or in chronic bronchitis. Gradual obstruction may be due to a bronchial tumour or pressure on a bronchus by, e.g., enlarged mediastinal lymph nodes, aortic aneurysm.