Ross & Wilson Anatomy and Physiology in Health and Illness (188 page)
Read Ross & Wilson Anatomy and Physiology in Health and Illness Online
Authors: Anne Waugh,Allison Grant
Tags: #Medical, #Nursing, #General, #Anatomy

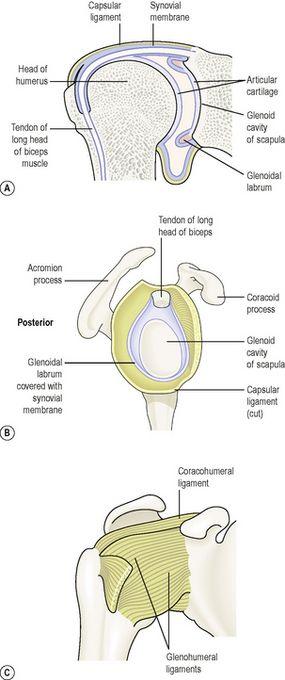
Figure 16.47
The right shoulder joint. A.
Section viewed from the front.
B.
The position of glenoidal labrum with the humerus removed, viewed from the side.
C.
The supporting ligaments viewed from the front.
Synovial membrane forms a sleeve round the part of the tendon of the long head of the biceps muscles within the capsular ligament and covers the glenoidal labrum.
The joint is stabilised partly by a number of ligaments (the glenohumoral, coracohumeral and transverse humeral) but mainly by the muscles (and their tendons) present in the shoulder. Certain of these muscles collectively are called the
rotator cuff
, and rotator cuff injury is a common cause of shoulder pain (
p. 425
). The stability of the joint may be reduced if these structures, together with the tendon of the biceps muscle, are stretched by repeated dislocations of the joint.
Muscles and movements (see
Fig. 16.65
)
The muscles that move the arm are described in more detail on
page 417
, and
Table 16.3
summarises the muscles and movements possible at the shoulder joint.
Table 16.3
Muscles and movements at the shoulder joint
| Extension | Latissimus dorsi, teres major |
| Flexion | Coracobrachialis, pectoralis major |
| Abduction | Deltoid |
| Adduction | Latissimus dorsi, pectoralis major |
| Lateral rotation | Teres minor, posterior part of deltoid |
| Medial rotation | Latissimus dorsi, pectoralis major, teres major and anterior part of deltoid |
| Circumduction | Combination of actions of above muscles |

Figure 16.65
The main muscles of the shoulder and upper limb. A.
Anterior view.
B.
Posterior view.
Elbow joint (
Fig. 16.48
)
This hinge joint is formed by the trochlea and the capitulum of the humerus, and the trochlear notch of the ulna and the head of the radius. It is an extremely stable joint because the humeral and ulnar surfaces interlock, and the capsule is very strong.
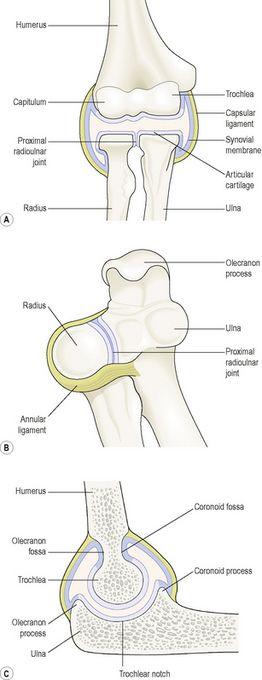
Figure 16.48
The elbow and proximal radioulnar joints. A.
Section viewed from the front.
B.
The proximal radioulnar joint, viewed from above.
C.
Section of the elbow joint, partly flexed, viewed from the side.
Extracapsular structures consist of anterior, posterior, medial and lateral strengthening ligaments, which contribute to joint stability.
Muscles and movements (see
Fig. 16.65
)
Because of the structure of the elbow joint, the only two movements it allows are flexion and extension. The biceps is the main flexor of the forearm, aided by the brachialis; the triceps extends it (
p. 417
).
Proximal and distal radioulnar joints
The
proximal radioulnar joint
is a pivot joint formed by the rim of the head of the radius rotating in the radial notch of the ulna, and is in the same capsule as the elbow joint. The
annular ligament
is a strong extracapsular ligament that encircles the head of the radius and keeps it in contact with the radial notch of the ulna (
Fig. 16.48B
).
The distal
radioulnar joint
is a pivot joint between the distal end of the radius and the head of the ulna (
Fig. 16.49
).
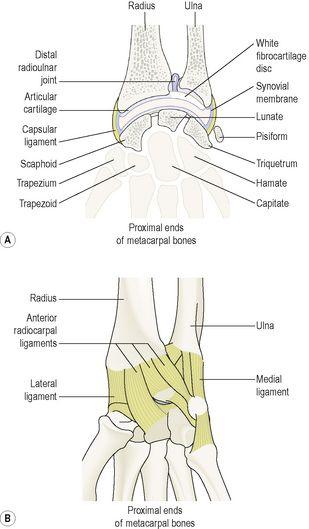
Figure 16.49
The wrist and distal radioulnar joints.
Anterior view.
A.
Section.
B.
Supporting ligaments.
Note, in addition, the presence of a fibrous membrane linking the bones along their shafts; this interosseous membrane is an example of a fibrous joint and prevents separation of the bones when force is applied at either end, i.e. at the wrist or elbow.
Muscles and movements (see
Fig. 16.65
)
The forearm may be pronated (turned palm down) or supinated (turned palm up). Pronation is caused by the action of the pronator teres (
p. 418
) and supination by the supinator and biceps muscles (
p. 418
).
Wrist joint (
Fig. 16.49
)
This is a condyloid joint between the distal end of the radius and the proximal ends of the scaphoid, lunate and triquetrum. A disc of white fibrocartilage separates the ulna from the joint cavity and articulates with the carpal bones. It also separates the inferior radioulnar joint from the wrist joint.
Extracapsular structures consist of medial and lateral ligaments and anterior and posterior radiocarpal ligaments.
Muscles and movements (see
Fig. 16.65
)
The wrist can be flexed, extended, abducted and adducted. The muscles that perform these movements are described in more detail on
page 417
.
Table 16.4
summarises the main muscles that move the wrist.
Table 16.4
Muscles and movements at the wrist joint
| Flexion | Flexor carpi radialis, flexor carpi ulnaris |
| Extension | Extensors carpi radialis (longus and brevis), extensor carpi ulnaris |
| Adduction | Flexor carpi radialis, extensor carpi radialis |
| Abduction | Flexor carpi ulnaris, extensor carpi ulnaris |
Joints of the hands and fingers
There are synovial joints between the carpal bones, between the carpal and metacarpal bones, between the metacarpal bones and proximal phalanges and between the phalanges. Movement at the hand and finger joints is controlled by muscles in the forearm and smaller muscles within the hand. There are no muscles in the fingers; finger movements are produced by tendons extending from muscles in the forearm and the hand.
The joint at the base of the thumb is a saddle joint, unlike the corresponding joints of the other fingers, which are condyloid. This means that the thumb is more mobile than the fingers and the thumb can be flexed, extended, circumducted, abducted and adducted. In addition, the thumb can be moved across the palm to touch the tips of each of the fingers on the same hand (opposition), an ability that confers great manual dexterity and allows, for example, the holding of a pen and the fine manipulation of objects held in the hand.
The joints between the metacarpals and finger bones allow movement of the fingers. The fingers may be flexed, extended, adducted, abducted and circumducted, with the first finger having the greatest flexibility of movement. The finger joints are hinge joints, and allow only flexion and extension.
The
flexor retinaculum
is a strong fibrous band that stretches across the front of the carpal bones, enclosing their concavity and forming the
carpal tunnel
. The tendons of flexor muscles of the wrist joint and the fingers and the median nerve pass through the carpal tunnel, the retinaculum holding them close to the bones. Synovial membrane forms sleeves around these tendons in the carpal tunnel and extends some way into the palm of the hand. Synovial sheaths also enclose the tendons on the flexor surfaces of the fingers. Their synovial fluid prevents friction that might damage the tendons as they move over the bones (
Fig. 16.50
).
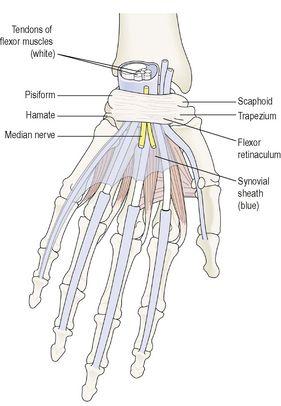
Figure 16.50
The carpal tunnel and synovial sheaths in the wrist and hand in blue; tendons in white.
Palmar view, left hand.
The
extensor retinaculum
is a strong fibrous band that extends across the back of the wrist. Tendons of muscles that extend the wrist and finger joints are encased in synovial membrane under the retinaculum. The synovial sheaths are less extensive than on the flexor aspect. The synovial fluid secreted prevents friction.
Hip joint (
Fig. 16.51
)