Ross & Wilson Anatomy and Physiology in Health and Illness (187 page)
Read Ross & Wilson Anatomy and Physiology in Health and Illness Online
Authors: Anne Waugh,Allison Grant
Tags: #Medical, #Nursing, #General, #Anatomy

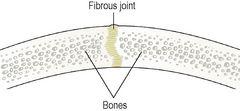
Figure 16.43
Suture (fibrous joint) of the skull.
Cartilaginous joints
These joints are formed by a pad of fibrocartilage, a tough material that acts as a shock absorber. The joint may be immovable, as in the cartilaginous epiphyseal plates, which in the growing child link the diaphysis of a long bone to the epiphysis (
p. 382
). In other joints, a limited degree of movement may take place, as between the vertebrae, which are separated by the intervertebral discs (
Fig. 16.44
), or at the symphysis pubis (
Fig. 16.37
), which is softened by circulating hormones during pregnancy to allow for childbirth.

Figure 16.44
The cartilaginous joint between adjacent vertebral bodies.
Synovial joints
Synovial joints are characterised by the presence of a space or capsule between the articulating bones (
Fig. 16.45
). The ends of the bones are held close together by a sleeve of fibrous tissue, and the capsule is lubricated with a small amount of fluid. Most synovial joints permit a range of movement.
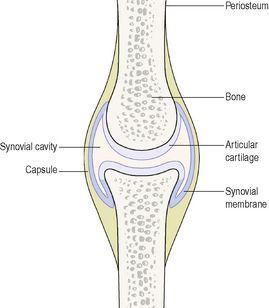
Figure 16.45
The basic structure of a synovial joint.
Characteristics of a synovial joint
All synovial joints have certain characteristics in common (
Fig. 16.45
).
Articular or hyaline cartilage
The parts of the bones which are in contact are always covered with hyaline cartilage (see
Fig. 3.20A, p. 38
). This provides a smooth articular surface, reduces friction and is strong enough to absorb compression forces and bear the weight of the body. The cartilage lining, which is up to 7 mm thick in young people, becomes thinner and less compressible with age. This leads to increasing stress on other structures in the joint. Cartilage has no blood supply and receives its nourishment from synovial fluid.
Capsule or capsular ligament
The joint is surrounded and enclosed by a sleeve of fibrous tissue which holds the bones together. It is sufficiently loose to allow freedom of movement but strong enough to protect it from injury.
Synovial membrane
This epithelial layer lines the capsule and covers all non-weight-bearing surfaces inside the joint. It secretes synovial fluid.
Synovial fluid
This is a thick sticky fluid, of egg-white consistency, which fills the synovial cavity. It:
•
nourishes the structures within the joint cavity
•
contains phagocytes, which remove microbes and cellular debris
•
acts as a lubricant
•
maintains joint stability
•
prevents the ends of the bones from being separated, as does a little water between two glass surfaces.
Little sacs of synovial fluid or
bursae
are present in some joints, e.g. the knee. They act as cushions to prevent friction between a bone and a ligament or tendon, or skin where a bone in a joint is near the surface.
Other intracapsular structures
Some joints have structures within the capsule, which assist in maintenance of stability, e.g. fat pads and menisci in the knee joint. When these structures do not bear weight they are covered by synovial membrane.
Extracapsular structures
•
Ligaments
that blend with the capsule provide additional stability at most joints.
•
Muscles
or their
tendons
also provide stability and stretch across the joints they move. When the muscle contracts it shortens, pulling one bone towards the other.
Nerve and blood supply
Nerves and blood vessels crossing a joint usually supply the capsule and the muscles that move it.
Movements at synovial joints
Movement at any given joint depends on various factors, such as the tightness of the ligaments holding the joint together, how well the bones fit and the presence or absence of intracapsular structures. Generally, the more stable the joint, the less mobile it is. The main movements possible are summarised in
Table 16.2
and
Figure 16.46
.
Table 16.2
Movements possible at synovial joints
| Movement | Definition |
|---|---|
| Flexion | Bending, usually forward but occasionally backward, e.g. knee joint |
| Extension | Straightening or bending backward |
| Abduction | Movement away from the midline of the body |
| Adduction | Movement towards the midline of the body |
| Circumduction | Movement of a limb or digit so that it describes the shape of a cone |
| Rotation | Movement round the long axis of a bone |
| Pronation | Turning the palm of the hand down |
| Supination | Turning the palm of the hand up |
| Inversion | Turning the sole of the foot inwards |
| Eversion | Turning the sole of the foot outwards |
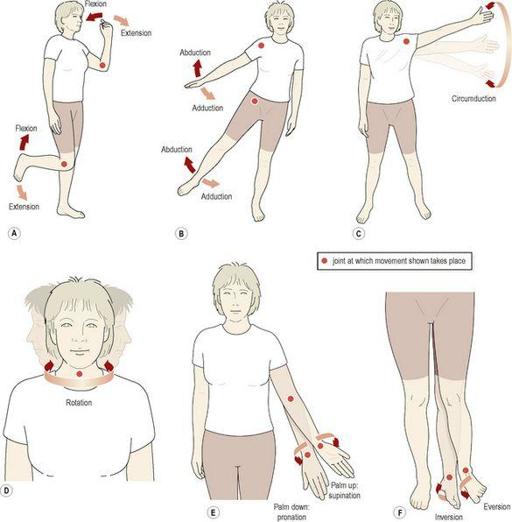
Figure 16.46
The main movements possible at synovial joints.
Types of synovial joint
Synovial joints are classified according to the range of movement possible (
Table 16.2
) or to the shape of the articulating parts of the bones involved.
Ball and socket joints
The head of one bone is ball-shaped and articulates with a cup-shaped socket of another. The joint allows for a wide range of movement, including flexion, extension, adduction, abduction, rotation and circumduction. Examples include the shoulder and hip.
Hinge joints
The articulating ends of the bones form an arrangement like a hinge on a door, and movement is therefore restricted to flexion and extension. The elbow joint is one example, permitting only flexion and extension of the forearm. Other hinge joints include the knee, ankle and the joints between the phalanges of the fingers and toes (interphalangeal joints).
Gliding joints
The articular surfaces are flat or very slightly curved and glide over one another, but the amount of movement possible is very restricted; this group of joints is the least movable of all the synovial joints. Examples include the joints between the carpal bones in the wrist, the tarsal bones in the foot, and between the processes of the spinal vertebrae (note that the joints between the vertebral bodies are the cartilaginous discs,
Fig. 16.44
).
Pivot joints
These joints allow a bone or a limb to rotate. One bone fits into a hoop-shaped ligament that holds it close to another bone and allows it to rotate in the ring thus formed. For example, the head rotates on the pivot joint formed by the dens of the axis held within the ring formed by the transverse ligament and the odontoid process of the atlas (
Fig. 16.22
).
Condyloid joints
A condyle is a smooth, rounded projection on a bone and in a condyloid joint it sits within a cup-shaped depression on the other bone. Examples include the joint between the condylar process of the mandible and the temporal bone, and the joints between the metacarpal and phalangeal bones of the hand, and between the metatarsal and phalangeal bones of the foot. These joints permit flexion, extension, abduction, adduction and circumduction.
Saddle joints
The articulating bones fit together like a man sitting on a saddle. The most important saddle joint is at the base of the thumb, between the trapezium of the wrist and the first metacarpal bone (
Fig. 16.35
). The range of movement is similar to that at a condyloid joint but with additional flexibility;
opposition
of the thumb, the ability to touch each of the fingertips on the same hand, is due to the nature of the thumb joint.
Main synovial joints of the limbs
Individual synovial joints have the characteristics described above, so only their distinctive features are included in this section.
Shoulder joint (
Fig. 16.47
)
This ball and socket joint is the most mobile in the body, and consequently is the least stable and prone to dislocation, especially in children. It is formed by the glenoid cavity of the scapula and the head of the humerus, and is well padded with protective bursae. The capsular ligament is very loose inferiorly to allow for the free movement normally possible at this joint. The glenoid cavity is deepened by a rim of fibrocartilage, the
glenoidal labrum
, which provides additional stability without limiting movement. The tendon of the long head of the
biceps muscle
is held in the intertubercular (bicipital) groove of the humerus by the transverse humeral ligament. It extends through the joint cavity and attaches to the upper rim of the glenoid cavity.