Ross & Wilson Anatomy and Physiology in Health and Illness (128 page)
Read Ross & Wilson Anatomy and Physiology in Health and Illness Online
Authors: Anne Waugh,Allison Grant
Tags: #Medical, #Nursing, #General, #Anatomy

The importance of nutrition is increasingly recognised as essential for health, and illness often alters nutritional requirements.
Malnutrition
This may be due to:
•
protein-energy malnutrition (PEM)
•
vitamin deficiencies
•
both PEM and vitamin deficiencies.
The degree of malnutrition can be assessed from measurement of body mass index (see
Box 11.1
).
Protein-energy malnutrition (
Fig. 11.2
)
This is the result of inadequate intake of protein, carbohydrate and fat. It occurs during periods of starvation and when dietary intake is inadequate to meet increased requirements, e.g. trauma, fever and illness. Infants and young children are especially susceptible as they need sufficient nutrients to grow and develop normally. If dietary intake is inadequate, it is not uncommon for vitamin deficiency to develop at the same time. Poor nutrition (malnutrition) reduces the ability to combat other illness and infection.
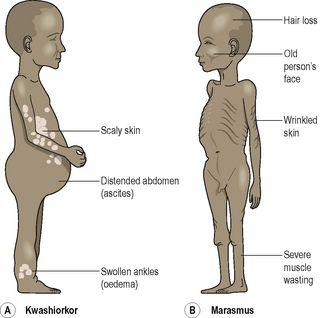
Figure 11.2
Features of protein-energy malnutrition.
Kwashiorkor
This is mainly caused by protein deficiency, and occurs in infants and children in some developing countries, especially when there has been serious drought and crop failure. Reduced plasma proteins lead to ascites and oedema (
p. 117
) in the lower limbs that masks emaciation. There is severe liver damage. Growth stops and there is loss of weight and loss of pigmentation of skin and hair accompanied by listlessness, apathy and irritability. Affected individuals are susceptible to infection and recovery from injury and infection takes longer.
Marasmus
This is caused by deficiency of both protein and carbohydrate. It is often caused by incorrect bottle feeding (overdilution of milk) or gastroenteritis, although people of any age can be affected. Marasmus is characterised by severe emaciation due to breakdown (catabolism) of muscle and fat. Growth is retarded, the skin becomes wrinkled due to absence of subcutaneous fat and hair is lost.
Malabsorption
The causes of malabsorption vary widely, from short-term problems such as gastrointestinal infections (
p. 317
) to chronic conditions such as cystic fibrosis (
p. 258
). Malabsorption may be specific for one nutrient, e.g. vitamin B
12
in pernicious anaemia (
p. 67
), or it may apply across a spectrum of nutrients, e.g. in tropical sprue (
p. 323
).
Obesity
In developed countries, this is a very common nutritional disorder in which there is accumulation of excess body fat. Clinically, obesity is present when body mass index exceeds 29.9 (see
Box 11.1
). It occurs when energy intake exceeds energy expenditure, e.g. in inactive individuals whose food intake exceeds daily energy requirements.
Obesity predisposes to:
•
gallstones (
p. 326
)
•
cardiovascular diseases, e.g. ischaemic heart disease (
p. 120
), hypertension (
p. 124
)
•
hernias (
p. 321
)
•
varicose veins (
p. 116
)
•
osteoarthritis (
p.424
)
•
type 2 (non-insulin dependent) diabetes mellitus (
p. 227
)
•
increased incidence of postoperative complications.
Conditions with dietary implications
In addition to nutritional disorder there are many conditions where dietary modifications are needed. Some of these are listed in
Box 11.3
.

Box 11.3
Conditions that require dietary modification
Obesity
Malnutrition
Diabetes mellitus (
p. 227
)
Diverticular disease (
p. 320
)
Coeliac disease (
p. 323
)
Phenylketonuria (
p. 435
)
Acute renal failure (
p. 345
)
Chronic renal failure (
p. 346
)
Liver failure (
p. 326
)
Lactose intolerance
For a range of self-assessment exercises on the topics in this chapter, visit
www.rossandwilson.com
Further reading
British Nutrition Foundation. The Eatwell Plate. Available online at
http://www.nutrition.org.uk/home.asp?siteId=43§ionId=299&which=1
. Accessed 21 January 2009
Department of Health. Dietary reference values of food energy and nutrients for the UK: COMA report. London: HMSO, 1991.
World Health Organization. Global database on body mass index. Available online at
http://www.who.int/bmi/index.jsp?introPage=intro_3.html
. Accessed 17 January 2009
CHAPTER 12
The digestive system
Organs of the digestive system
279
Alimentary canal
279
Accessory organs
279
Basic structure of the alimentary canal
279
Adventitia or serosa
279
Muscle layer
280
Submucosa
281
Mucosa
281
Nerve supply
281
Mouth
283
Tongue
283
Teeth
284
Salivary glands
285
Structure of the salivary glands
286
Secretion of saliva
286
Functions of saliva
286
Pharynx
287
Oesophagus
287
Structure of the oesophagus
288
Functions of the mouth, pharynx and oesophagus
288
Stomach
289
Structure of the stomach
289
Gastric juice and functions of the stomach
291