Ross & Wilson Anatomy and Physiology in Health and Illness (135 page)
Read Ross & Wilson Anatomy and Physiology in Health and Illness Online
Authors: Anne Waugh,Allison Grant
Tags: #Medical, #Nursing, #General, #Anatomy

Swallowing (deglutition) (
Fig. 12.16
)
This occurs in three stages after chewing is complete and the bolus has been formed. It is initiated voluntarily but completed by a reflex (involuntary) action.
1.
The mouth is closed and the voluntary muscles of the tongue and cheeks push the bolus backwards into the pharynx.
2.
The muscles of the pharynx are stimulated by a reflex action initiated in the walls of the oropharynx and coordinated in the medulla and lower pons in the brain stem. Involuntary contraction of these muscles propels the bolus down into the oesophagus. All other routes that the bolus could take are closed. The soft palate rises up and closes off the nasopharynx; the tongue and the pharyngeal folds block the way back into the mouth; and the larynx is lifted up and forward so that its opening is occluded by the overhanging epiglottis preventing entry into the airway (trachea).
3.
The presence of the bolus in the pharynx stimulates a wave of peristalsis that propels the bolus through the oesophagus to the stomach.
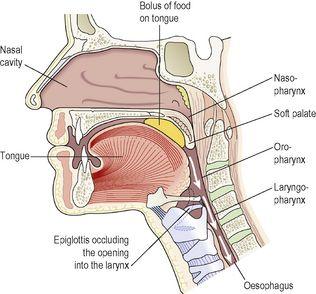
Figure 12.16
Section of the face and neck showing the positions of structures during swallowing.
Peristaltic waves pass along the oesophagus only after swallowing begins (see
Fig. 12.4
). Otherwise the walls are relaxed. Ahead of a peristaltic wave, the cardiac sphincter guarding the entrance to the stomach relaxes to allow the descending bolus to pass into the stomach. Usually, constriction of the cardiac sphincter prevents reflux of gastric acid into the oesophagus. Other factors preventing gastric reflux include:
•
the attachment of the stomach to the diaphragm by the peritoneum
•
the maintenance of an acute angle between the oesophagus and the fundus of the stomach, i.e. an acute cardio-oesophageal angle
•
increased tone of the cardiac sphincter when intra-abdominal pressure is increased and the pinching effect of diaphragm muscle fibres.
The walls of the oesophagus are lubricated by mucus which assists the passage of the bolus during the peristaltic contraction of the muscular wall.
Stomach

Learning outcomes
After studying this section, you should be able to:
describe the location of the stomach with reference to surrounding structures
The stomach is a J-shaped dilated portion of the alimentary tract situated in the epigastric, umbilical and left hypochondriac regions of the abdominal cavity.
Organs associated with the stomach (
Fig. 12.17
)
Anteriorly
– left lobe of liver and anterior abdominal wall
Posteriorly
– abdominal aorta, pancreas, spleen, left kidney and adrenal gland
Superiorly
– diaphragm, oesophagus and left lobe of liver
Inferiorly
– transverse colon and small intestine
To the left
– diaphragm and spleen
To the right
– liver and duodenum.
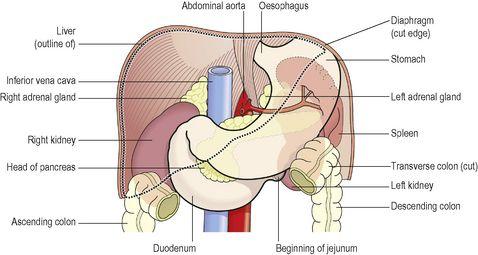
Figure 12.17
The stomach and its associated structures.
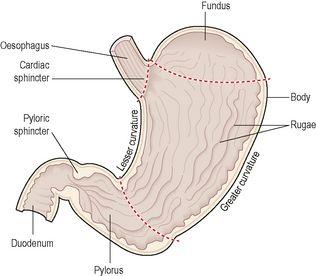
Structure of the stomach (
Fig. 12.18
)
The stomach is continuous with the oesophagus at the cardiac sphincter and with the duodenum at the pyloric sphincter. It has two curvatures. The
lesser curvature
is short, lies on the posterior surface of the stomach and is the downward continuation of the posterior wall of the oesophagus. Just before the pyloric sphincter it curves upwards to complete the J shape. Where the oesophagus joins the stomach the anterior region angles acutely upwards, curves downwards forming the
greater curvature
and then slightly upwards towards the pyloric sphincter.