The Ghost in My Brain (23 page)
Read The Ghost in My Brain Online
Authors: Clark Elliott

I tested normal on the Padula midline test. But as we have seen from previous chapters, I experienced every one of these rather startling symptomsâfor reasons other than a midline shiftâon a regular basis, suggesting that there were other problems to be found with my ambient visual system.
Next, in the
Yoked Prism Walk
, Martha gave me a pair of thick prism goggles to wear, and then observed my gait as I walked down the hallway and back four times. Before each trip she adjusted the goggles to a different orientation.
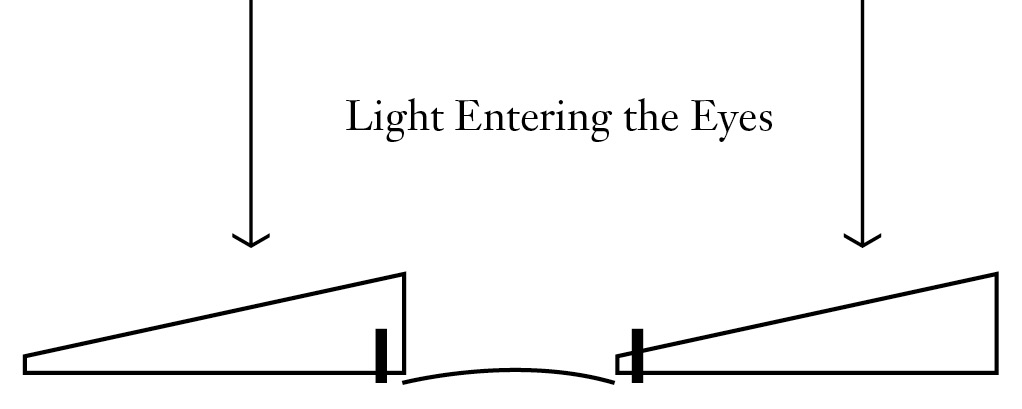
Figure 12:
Prism GlassesâTop View with the Yoked Prisms Shifting Images to the Left
Experientially, prism lenses bend the room in a “fun house” way, tilting it up, sloping it down, and bending the top and bottom in a great arc to the left or to the right, depending on the orientation of the prisms. (“Yoked” means that the prisms are oriented in the same direction.) Although in all cases the visual scene will look altered, patients may have widely differing abilities to walk down the hall from one orientation to another. In my case bending the floor up, and tilting it down, or bending the light from the right, was slightly disorienting, but I was almost immediately able to adjust and navigate the hallway. When the light was bent from my left, though, I became completely disoriented: I had trouble walking and I ran into the side of an open doorway along the way. Such difficulty with one of the lateral orientations is typical for TBI sufferers.
In writing about this test, Zelinsky explains that the Yoked Prism Walk evaluates gross body movements at a reflexive level, as well as spatial orientation,
while the patient is moving.
It
can demonstrate how poor stability may impair higher-level perception.
*
The distinct discrepancy between my performance with the prisms bending the light left versus bending it right was importantâespecially when linked to the similar problem I reported, in my notes, of growing dizzy when turning around in one direction, but not the other. This may also have been linked to the phenomenon, discussed earlier, that under brain stress, I was unable to turn to my right at all: I simply could not conceive of “right-ness.” And, it may explain other anecdotal aspects of my life as well. For example, if I went running with my daughter, I had to orient
myself
on her left side; when I was on her right, I would start to get dizzy almost immediately.
*
Martha next gave me an
Asymmetrical Tonic Neck Reflex
(ATNR) test. “Stand up and hold your arms out in front of you,” she said, “like Frankenstein, with your fingers extended . . . Okay. Good. Now turn your head to the left, and then to the right.”
ATNR is an innate survival reflex, seen in infants, which often reemerges in adults as a protective mechanism after a shock to the nervous system, such as from TBI. If the subject lowers his opposite arm when turning his head, this suggests a shock has occurred. In my case, an ATNR was present when I turned my head to the left.
Martha then assessed my extraocular musclesâthe six muscles that move the eyeâusing
pursuit tests
, where I tracked the eraser-end of a pencil with my eyes while keeping my head still. She had me follow various patterns, including a big
H
. Martha was looking for any partial paralysis in my eye movements, and also observing my anticipatory eye movements in predicting the path of the targetâwhich gave clues to the peripheral awareness in my brain. Was I able, without thinking about it, to predict the path the eraser was going to take, and adjust my eyes to smoothly follow that predicted path? In my case I had no problem following the pencil, even though, as we saw previously, following a baseball when playing with my boys was extremely fatiguing. The pursuit test results would prove to be important in interpreting the results of later tests.
Martha next gave me a
Near Point of Convergence
test by bringing the pencil close to the bridge of my nose, and then, afterward, the
LANG-STEREOTEST II
to check my stereoscopic vision and depth perceptionâboth of which tested normal.
Lastly, Martha gave me a
King-Devick
Test
, in which I read a series of single-digit numbers on two pages. One of the pages just had the numbers on a white background, and the other had lines inserted between one number and the next. The test is used to look for deficiencies in
saccadic eye movements
(extremely rapid, intentional, simultaneous movements of both eyes in the same direction), which can be an indicator of TBI. Tests like this are often used to obtain a quick, objective sideline diagnosis of concussion in football players and other athletes. I tested normal on this exam.
In between completing her work with other patients, Zelinsky would check in with Martha and review some of the data Martha had been collecting. After an hour Zelinsky had me move to her examination room and sit in the phoropter chair, where she began her own testing.
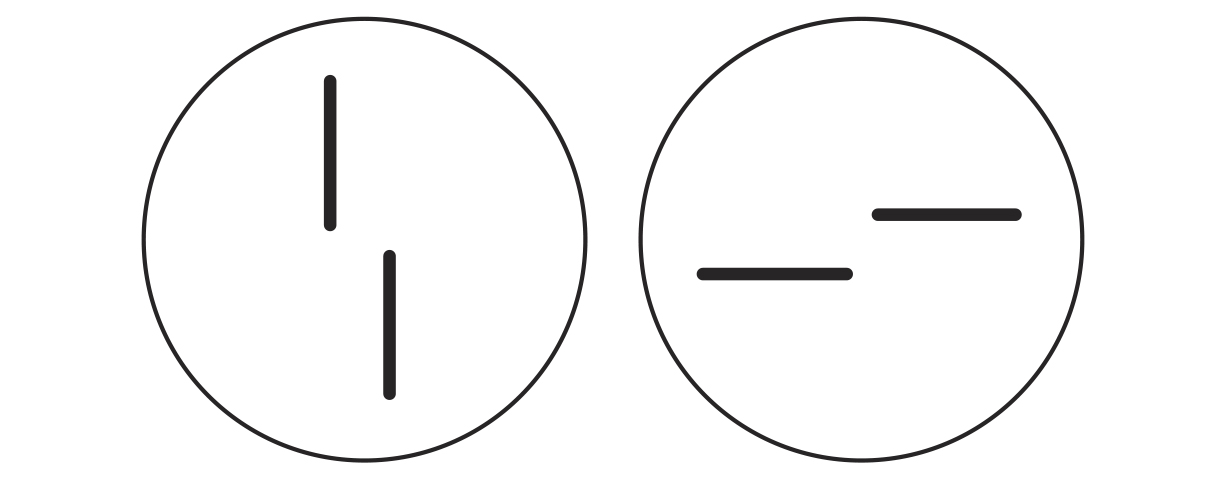
Figure 13:
Fixation Disparity Test
One of the first tests Zelinsky gave me is called the
Super Fixation Disparity Test
©
â
named after its designer, Dr. Selwyn Super (D.O., F.A.A.O., Ph.D.).
*
Fixation disparity occurs when the two elements of binocular vision are out of sync.
To get the idea of fixation disparity, consider the circle on the left in
Figure 13
. Note that in the circle there are two vertical line segmentsâone in the top hemisphere, and one in the bottom. Using occlusions, we arrange it so that each line is seen by only one eye. The measure of misalignment is determined by how far these lines appear to be offset from each other. Testing for disparity is also done horizontally in the same way using the second circle.
*
Some alignment disparity is useful as part of the design of the stereo vision system. If monocularly viewed targets are incorrectly misaligned when a person is attempting to view a
scene in the real world, the binocular visual system can usually bring them into alignment and thus avoid double vision. But this is fatiguing, and causes cognitive difficultiesâbecause we are continually refocusing on near and far objects throughout the day, and binocular readjustments have to be made each time. Zelinsky looks to see how much misalignment patients can tolerate in either direction before they lose the ability to synthesize a single stereo image from the two sets of input.
It is believed that in some cases, if such alignment is habitually too far off, the brain will simply shut down the confusing signals from one of the eyes. When this happens it may be true that cognitive functioning in the 3D visual/spatial “internal world” of symbols is also diminished, effectively reducing one's ability to perform complex reasoning and problem solving.
Next, Zelinsky gave me the related
Von Graefe Phoria Test
. Similar to the Super test, Von Graefe measures the habitual tendency of the eyes to point inward, or outward, in the absence of a point on which they can both fixate. Phoria has implications for binocular vision, and the latency period during which the eyes are interpreting binocular visual signals. The test is performed using the phoropter by keeping the image for one eye still, and slowly moving another identical image until the subject reports them as being aligned.
On the Super Fixation Disparity Test©, which takes place in free space (e.g., as per discussion above, all of our “one hundred” imaginary pathways are available from the retina to the visual cortex), Zelinsky found that my overall habitual eye position was slightly outward, though still within the normal range. But on the Von Graefe Phoria Test, which blocks off much of the peripheral vision (so that now only “fifty” pathways are available), she found that my habitual eye aiming was
perturbed: my eyes were pointed inward at a distance, and way outward when focused on close-up objects. This caused an exhausting lag in cognition as my eyes had to continually re-aim to avoid double vision. We can imagine the corollary of trying to follow a conversation between two people when, every time we shift our gaze from one person to the other, the audio lags behind the movement of their mouths for a second or two while we struggle to get it to catch up to their gestures.
Next, Zelinsky gave me a
Visual Localization Test.
In this simple (but in my case, ultimately quite telling) test, Zelinsky held a pencil so that the eraser was facing me, about twenty inches in front of my eyes. She said, “Look at the pencil. Then close your eyes and, without looking, reach up and touch it with your fingertip.”
She repeated the test with the target in a number of different positions, and also several times specifically had me reach across my body and touch the target with my opposite hand. Despite the theoretical ease of the task, I was completely unable to find the eraser tip of the pencil, with my eyes closed, in any of the positions, helplessly waving my finger around in space until I accidentally hit the target.
In general, a subject's inability to touch the eraser can be caused by three distinct failures. First, the subject may simply not know
where
the eraser is; his central vision allows him to
see
it fine, so he knows
what
it is, but his peripheral vision does not allow him to find it in space relative to his body. Second, the subject might know where the eraser isâhis peripheral vision is working fineâbut he doesn't know where his hand is. For example, if the subject can reach the eraser on his right-hand side with either arm, but not when the eraser is on his left-hand side, the problem is likely with his visual processing.
If the subject can accurately locate the eraser on either side with one arm, but not the other arm, then the problem is likely with the proprioceptive signals coming from his body. Or, third, in the worst case, he could have problems with both.
In my case, the vision signals going to my visual cortex were fine (eyesight)âthis was not the problem. Thus we knew that it had to be the signals coming
from
my muscles, the “where I am” sense, which were not getting through correctly to form an accurate body image in my brain. Zelinsky had two additional clues in interpreting this failure: first, she noted that my severe neck and head pain suggested a compromised motor response sending conflicting signals to my various neck, arm, and back muscles; and second, Martha had noted the ATNR present when I turned my head, indicating that my neck was not operating independently of my shoulders.
Zelinsky followed up with a
Confrontation Visual Field Exam.
She held her hand out to the left side of my head, outside the range of peripheral vision, and said, “Cover your right eye, look straight ahead at my eyes, and tell me when you see my fingers moving.” She began wiggling her fingers, at the same time slowly bringing her hand toward the center of my face. As soon as I signaled that I could see her fingers wiggling, she repeated the test on the other side. Zelinsky was determining the volume of space to which I could attend, and was measuring the signals going into my visual system, looking for possible damage to my ganglion cells.
Because I had performed well on the H-pursuit test, successfully anticipating the movement of the pencil through the
H
pattern in the normal way, because my King-Devick Test was normal, and because I demonstrated normal peripheral awareness on the Confrontation Visual Field Exam, Zelinsky
knew that the problem was not likely to be with the eyesight system itself.
Lastly, Zelinsky took me through her patented
Z-Bell⢠Test
. The first time one experiences this test, it is quite stunning, and seems almost impossibly magical. While I was sitting in her optometry chair, Zelinsky said, “Close your eyes. When I ring the bell, reach out and touch it with your finger.” After my eyes were closed, she brought out a series of differently pitched bells and rang them in various quadrants, high and low, left and right. The test feels
weird
because, with your eyes closed, you can't see anything, so it seems as if you aren't “using” your eyes. And yet, depending on which lenses, tints, and occlusions she uses to alter the light striking your
closed
eyelids, sometimes your hand just waves around helplessly, but at other times you can “feel” exactly where the bell is, and touch itâlike feeling the “power of the force” in a
Star Wars
movie.