Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis (166 page)
Authors: Mary A. Williamson Mt(ascp) Phd,L. Michael Snyder Md

BOOK: Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis
3.14Mb size Format: txt, pdf, ePub
Magnetic resonance imaging (MRI): Sensitivity is superior to CT scanning for mass lesions.
The advantages include lack of ionizing radiation and different planes of imaging.
• It is the technique of choice to look for hemangiomas.
• It is useful in distinguishing between a regenerating nodule and a tumor in the cirrhotic liver.
• MRI can be used to monitor the liver for iron and copper deposition and, with some modification, can identify fatty liver and can produce an estimated quantification of fat content.
• It can sometimes detect Budd-Chiari syndrome (hepatic vein thrombosis) without the need for IV iodinated contrast media (gadolinium is required).
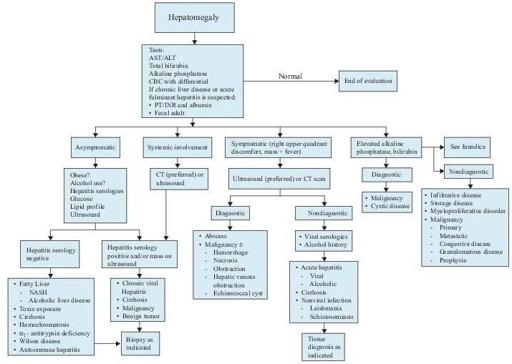
Figure5–6
Algorithm for the workup of hepatomegaly, if the vertical span is > 12 cm by physical examination or imaging. ALT, alanine aminotransferase; AST, aspartate aminotransferase; CBC, complete blood count; CT, computed tomography; FOBT, fecal occult blood test; GI, gastrointestinal; INR, international normalized ratio; NASH, nonalcoholic steatohepatitis; PT, prothrombin time.
Other books
Then Came You by Vanessa Devereaux
How to Stay Married by Jilly Cooper
Monsters by Liz Kay
Ashes by Now by Mark Timlin
One Night in Mississippi by Craig Shreve
Rock Me All Night by Katherine Garbera
Project Best Friend by Chrissie Perry
Alexander & Rebecca (Royals of Valleria #1) by Knightly, Marianne
An Ace Up My Sleeve by James Hadley Chase
The TROUBLE with BILLIONAIRES: Book 2 by Kristina Blake