Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis (65 page)
Authors: Mary A. Williamson Mt(ascp) Phd,L. Michael Snyder Md

BOOK: Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis
6.86Mb size Format: txt, pdf, ePub
Definition
Hyperlipidemia is an elevation of lipids (cholesterol, cholesterol esters, phospholipids, and triglycerides) in the bloodstream; is a risk factor for coronary heart disease (CHD); and promotes atherosclerosis. Lipids are transported as lipoproteins in the body; there are five major types: chylomicrons, VLDLs, intermediate-density lipoproteins (IDLs), LDLs, and HDLs. The protein portions of the lipoprotein are referred as apolipoprotein, of which there are six major classes (A, B, C, D, E, and H) and numerous subclasses (AI, AII, AIV, AV, B48, B200, CI, CII, CIII, and CIV).
3-2
).
3-3
).
TABLE 3–2 Diseases That May Cause Dyslipidemia and Associated Lipid Changes
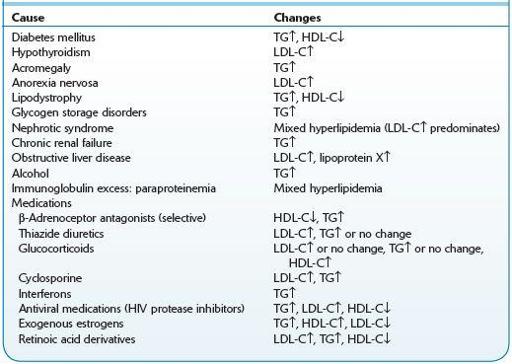
HDL-C, high-density lipoprotein–cholesterol; LDL-C, low-density lipoprotein–cholesterol; TG, triglyceride; ↑, increased levels; ↓, decreased levels.
TABLE 3–3 Classificationof Familial Dyslipidemias According to Predominant Lipid Abnormality and Etiology
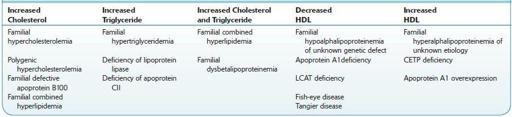
CETP,cholesterylestertransportprotein;HDL,high-densitylipoprotein;LCAT,lecithin–cholesterolacyltransferase;TG,triglyceride.
Low-risk persons: Further testing is not required if the HDL-cholesterol level is ≥40 mg/dL and TC is <200 mg/dL.
Other books
A Poor Relation by Carola Dunn
The Familiars by Adam Jay Epstein
The life of Queen Henrietta Maria by Taylor, Ida A. (Ida Ashworth)
Venetian Masquerade by Suzanne Stokes
From Here to There by Rain Trueax
Breakout by Ann Aguirre
Sunspire (The Reach, Book 4) by Mark R. Healy
The Stories of Ray Bradbury by Ray Bradbury
Last Chance by Victoria Zagar
Hell Bent by William G. Tapply