My Stroke of Insight: A Brain Scientist's Personal Journey (4 page)
Read My Stroke of Insight: A Brain Scientist's Personal Journey Online
Authors: Jill Bolte Taylor
Tags: #Heart, #Cerebrovascular Disease, #Diseases, #Health & Fitness, #Body; Mind & Spirit, #Medical, #Biography, #Cerebrovascular Disease - Patients - United States, #Rehabilitation, #United States, #Brain, #Patients, #Personal Memoirs, #Taylor; Jill Bolte - Health, #Biography & Autobiography, #Neuroscience, #Cerebrovascular Disease - Patients - Rehabilitation, #Science & Technology, #Nervous System (Incl. Brain), #Healing

Similar to vision, our ability to hear sound also depends upon our detection of energy traveling at different wavelengths. Sound is the product of atomic particles in space colliding with one another and emitting patterns of energy. The energy wavelengths, created by the bombarding particles, beat upon the tympanic membrane in our ear. Different wavelengths of sound vibrate our eardrum with unique properties. Similar to our retinal cells, the hair cells of our auditory Organ of Corti translate this energy vibration in our ear into a neural code. This eventually reaches the auditory cortex (in the temporal region of our brain) and we hear sound.
Our most obvious abilities to sense atomic/molecular information occur through our chemical senses of smell and
taste. Although these receptors are sensitive to individual electromagnetic particles as they waft past our nose or titillate our taste buds, we are all unique in how much stimulation is required before we can smell or taste something. Each of these sensory systems is also made up of a complex cascade of cells, and damage to any portion of the system may result in an abnormal ability to perceive.
Finally, our skin is our largest sensory organ, and it is stippled with very specific sensory receptors designed to experience pressure, vibration, light touch, pain, or temperature. These receptors are precise in the type of stimulation they perceive such that only cold stimulation can be perceived by cold sensory receptors and only vibration can be detected by vibration receptors. Because of this specificity, our skin is a finely mapped surface of sensory reception.
The innate differences we each experience in terms of how sensitive we are to different types of stimulation contribute greatly to how we perceive the world. If we have problems hearing when people speak, then we will hear only bits and pieces of conversation and make decisions and judgments based upon minimal information. If our eyesight is poor, then we will focus on fewer details and our interaction with the world will be affected. If our sense of smell is deficient, then we may not be able to discriminate between a safe environment and a health hazard, rendering us more vulnerable. At the opposite extreme, if we are oversensitive to stimulation, we may avoid interacting with our environment and miss out on life's simple pleasures.
Pathology and disease of the mammalian nervous system generally involves the brain tissue that distinguishes that specific species from other species. Consequently, in the case of the human system, the outer layers of our cerebral cortex are often vulnerable to disease. Stroke is the number one disabler in our society and the number three killer.
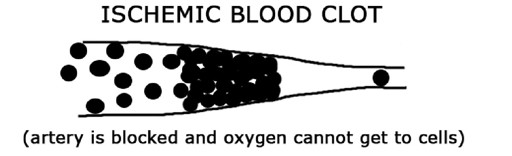
Because neurological disease often involves the higher cognition layers of our cerebral cortex, and because stroke occurs four times more frequently in the left cerebral hemisphere, our ability to create or understand language is often compromised. The term stroke refers to a problem with the blood vessels carrying oxygen to the cells of the brain, and there are basically two types: ischemic (ih-skee-mik) and hemorrhagic (hem-o-radg-ik).
According to the American Stroke Association, the ischemic stroke accounts for approximately 83% of all strokes. Arteries carry blood into the brain and their shape tapers smaller and smaller as they travel farther away from the heart. These arteries carry life-supporting oxygen necessary for cells, including neurons, to survive. With ischemic stroke, a blood clot travels into the artery until the tapered diameter of the artery becomes too small for the clot to pass any farther. The blood clot blocks the flow of oxygen-rich blood to the cells beyond the point of obstruction. Consequently, brain cells become traumatized and often die. Since neurons generally do not regenerate, the dead neurons are not replaced. The function of the deceased cells may be lost permanently, unless other neurons adapt over time to carry out their function. Because every brain is unique in its neurological wiring, every brain is unique in its ability to recover from trauma.
The hemorrhagic stroke occurs when blood escapes from the arteries and floods into the brain. Seventeen percent of all strokes are hemorrhagic. Blood is toxic to neurons when it comes in direct contact with them, so any leak or
vascular blowout can have devastating effects on the brain. One form of stroke, the aneurysm (an-yu-rism), forms when there is a weakening in the wall of a blood vessel that consequently balloons out. The weakened area fills with blood and can readily rupture, spewing large volumes of blood into the skull. Any type of hemorrhage is often life threatening.

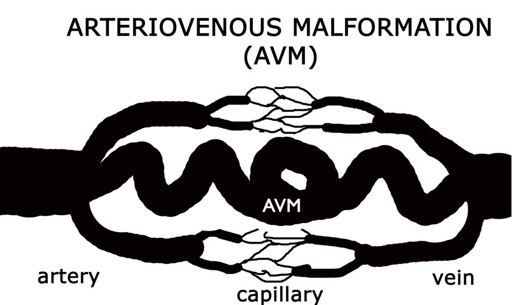
An arteriovenous malformation (AVM) is a rare form of hemorrhagic stroke. It is a congenital disorder whereby an individual is born with an abnormal arterial configuration. Normally, the heart pumps blood through arteries with high pressure while blood is retrieved through veins, which are low pressure. A capillary bed acts as a buffering system or neutral zone between the high-pressure arteries and the low-pressure veins.

In the case of the AVM, an artery is directly connected to a vein with no buffering capillary bed in between. Over time, the vein can no longer handle the high pressure from
the artery and the connection between the artery and vein is broken - sp
illin
g blood into the brain. Although the AVM accounts for only 2% of all hemorrhagic strokes,
3
it is the most common form of stroke that strikes people during their prime years of life (ages 25-45). I was 37 when my AVM blew.
Regardless of the mechanical nature of the vascular problem, be it a blood clot or a hemorrhage, no two strokes are identical in their symptoms because no two brains are absolutely identical in their structure, connections or ability to recover. At the same time, it is impossible to talk about the symptoms resulting from stroke without having a conversation about the innate differences between the right and left cerebral hemispheres. Although the anatomical structure of the two hemispheres is relatively symmetrical, they are quite diverse in not only how they process information, but also in the types of information they process.
The better we understand the functional organization of the two cerebral hemispheres, the easier it is to predict what deficits might occur when specific areas are damaged. Perhaps more important, we might gain some insight into what we can do to help stroke survivors recover lost function.
WARNING SIGNS OF STROKE
S
= SPEECH, or any problems with language
T
= TINGLING, or any numbness in the body
R
= REMEMBER, or any problems with memory
O
= OFF BALANCE, problems with coordination
K
= KILLER HEADACHE
E
= EYES, or any problems with vision
STROKE
is a medical emergency. Call 9-1-1
Second College Edition (Boston: Houghton Mifflin Company, 1985)
Derek E. Wildman, et.al., Center for Molecular Medicine and Genetics Department of Anatomy and Cell Biology, Wayne State University School of Medicine (Accessed September 10, 2006), <
http://www.pnas.org/cgi/content/full/100/12/7181
>
National Institute of Neurological Disorders and Stroke (Accessed September 10, 2006), <
http://www.ninds.nih.gov
>

Scientists have been studying the functional asymmetries of the human cerebral cortices for over 200 years. To my knowledge, the first person on record to suggest that each hemisphere actually had its own mind was Meinard Simon Du Pui. In 1780, Du Pui claimed that mankind was
Homo Duplex
- meaning that he had a double brain with a double mind.
10
Nearly a century later, in the late 1800s, Arthur Ladbroke Wigan witnessed the autopsy of a man who could walk, talk, read, write, and function like a normal man. Upon examination of his brain, however, Wigan discovered that this man had only one cerebral hemisphere. Wigan concluded that since this man, who had only "half" a brain, had a whole mind and could function like a whole man, then those of us who have two hemispheres must have two minds. Wigan enthusiastically championed this "Duality of the Mind" theory.
11
Over the centuries, various conclusions have been drawn about the differences and similarities in how the two hemispheres process information and learn new material. This subject gained tremendous popularity in the United States in the 1970s, following a series of split-brain experiments where Dr. Roger W. Sperry surgically cut the fibers of the corpus callosum of people experiencing severe epileptic seizures. In his 1981 Nobel lecture, Sperry commented: