Oxford Handbook of Midwifery (140 page)
Read Oxford Handbook of Midwifery Online
Authors: Janet Medforth,Sue Battersby,Maggie Evans,Beverley Marsh,Angela Walker

- The position should be sustainable for both the mother and the baby.
Support may sometimes be required to assist good positioning. This may be in the form of cushions to support a comfortable position for the mother or to raise the baby to the level of the breast.
The following should be avoided:
- Holding the back of the baby’s head—this will cause the baby to push their head backwards away from the breast
- Holding the breast away from the baby’s nose—this can disturb the attachment and also prevent drainage from some lobes of the breast
- Holding the baby in a bottle-feeding position—this necessitates the baby to turn their head, which can cause friction to the nipple
- Taking the breast down to the baby rather than bringing the baby to the breast—this alters the shape of the breast and can cause problems, including ineffective suckling by the baby and backache for the mother.
Biological nurturing
This is a new, non-prescriptive, mother-centred breastfeeding approach that refers to a range of semi-reclined maternal breastfeeding postures and innate feeding behaviours.
5
The positions used are similar to those used in skin-to-skin contact. The baby is held instinctively and cuddled in a natural way. This can be done with the baby held long ways, sideways or slanting. The baby always has close contact with the breast and can have unrestricted access to the breast for feeding. This is a useful approach for many mothers and especially those encountering problems with latching on. The Baby Friendly Initiative (BFI) recommends that those working towards BFI accreditation should inform themselves about biological nur- turing and to look for ways to incorporate this information within a frame- work of care that provides women with a range of skills to enable them to adapt their breastfeeding to a variety of situations.
6Attachment of the baby at the breast
Attachment is the term used to describe how the baby’s mouth fits around
the mother’s nipple and areola to suckle at the breast.
7 The three main reflexes required for a baby to attach effectively are:
The three main reflexes required for a baby to attach effectively are: - Rooting reflex
- Sucking reflex
- Swallowing reflex.
If any of these reflexes is absent, the baby will not be able to attach and feed effectively. Premature babies frequently are unable to coordinate the reflexes.
Process of attachment
In order to attach correctly, the baby needs to:
- Open their mouth in a wide gape with their tongue down and forward (Fig. 24.1)
- The lower lip, then the tongue, should be the first point of contact
- The first contact should be well away from the base of the nipple
- They should then reach up and bring their mouth over the nipple, taking in a large portion of breast tissue to form the teat (Fig. 24.2).
664
CHAPTER 24
Breastfeeding
Fig. 24.1
The baby should be encouraged to open their mouth widely.
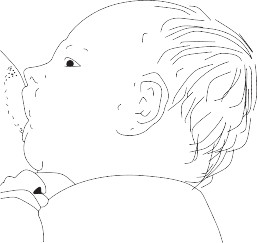
Fig. 24.2
Baby correctly attached at the breast.MANAGEMENT OF BREASTFEEDING
665
Recognizing correct attachment
- The baby’s mouth is wide open (wider than 100°) and they have a large mouthful of breast.
- The chin should indent the breast.
- There should be more areola visible above his top lip than below the baby’s bottom lip.
- The nose should be close to the breast but not squashed.
- The cheeks are round and full.
- The whole of the lower jaw moves.
- The lower lip is curled outwards but this is not always easily visible if the baby is close to the breast.
- The mother feels a strong, and sometimes uncomfortable, ‘drawing’ sensation as the baby scoops up the nipple and breast tissue, draws it into his or her mouth and commences suckling.
- Swallowing may be heard but this only indicates that milk is flowing, not that the positioning and attachment are correct.
Exaggerated attachment at the breast
This is useful if:
- The baby is unable to attach and feed effectively
- The baby has a ‘tongue tie’ and has difficulty staying attached
- The baby has a cleft palate
- The baby is premature
- The nipples are sore or cracked and feeding is almost unbearable.
How to attain an exaggerated attachment
If the mother is going to feed from her left breast, she needs to cup the breast underneath with her left hand, keeping her fingers well away from the areola. There is always a tendency to want to move the fingers up, but this will affect the success of the attachment. The thumb should tilt the nipple back so it looks like it is pointing away from the baby. This will have the effect of making the breast under the nipple bulge forwards. The
baby’s bottom lip should make contact with the breast well away from the
 base of the nipple.
base of the nipple.Pattern of sucking
Normally once the baby is attached he or she will take a few quick sucks at the breast which will initiate the oxytocin reflex. As the milk begins to flow and fills the mouth, the baby’s sucks will become slower and deeper. The baby will pause occasionally. If a baby continues to take frequent short sucks or there are audible ‘smacking’ noises as the baby sucks, this is a good indication that the attachment is incorrect.
Recognizing incorrect attachment
- The mouth is not wide open.
- The bottom lip is not curled outwards, or it is less curled than the upper lip.
- There is the same amount of areola below the bottom lip as above the top lip.
- There is a gap between the breast and the chin.
- The nose is either squashed into the breast or a wide distance from the breast.
CHAPTER 24
Breastfeeding666
- The cheeks are drawn in as the baby sucks.
- The breast tissue is puckered.
- The breast tissue moves in and out of the baby’s mouth as he feeds.
- The baby makes little sucks as if he is sucking a dummy.
- There is no change in the rhythm of feeding.
- The baby will show frustration at not having his hunger satisfied, by either becoming sleepy and ceasing to suck or by coming off the breast and crying.
- The colour of the stools may change back to green/brown from yellow.
Results of ineffective attachment
The mother may:
- Feel pain when feeding
- Experience sore nipples, especially cracks across the tip of the nipple or at the base of the nipple
- Experience engorgement of the breast. The baby may:
- Appear unsatisfied
- Cry a lot and want frequent feeds, or may feed for protracted lengths of time
- Receive insufficient milk and fail to gain or even lose weight
- Become frustrated and refuse to feed
- Receive adequate nourishment for the first few weeks by feeding frequently if the oxytocin reflex works well but then will fail to thrive.
Measures shown to enhance breastfeeding success
A comprehensive systematic review conducted by NICE
8
has identified what practices enable a mother to breastfeed for longer, and these should be used in conjunction with the following information.Baby-led feeding

Baby-led feeding, or demand feeding, simply consists of feeding the baby whenever he or she wishes and for as long as he or she wishes.
There is substantial evidence that the timing and duration of breastfeeds should be responsive to the needs of the baby.
9
Babies will feed at the breast for very different lengths of time if left undisturbed, and it is thought that the length of a feed is determined by the rate of milk transfer between mother and baby.
10Limiting the duration of the feed or removing a baby from the breast before they finish spontaneously, may prevent the baby from receiving adequate calorific intake causing failure to gain weight despite frequent feeds and an apparently good milk supply.
Unrestricted frequency of feeds is also advocated. Observation studies have demonstrated that the frequency of feeds in the first few weeks appears to be unpredictable and random, varying between 1h and 8h. Babies who regulate the length and frequency of feeds gain weight more quickly.
Advice to the mother to restrict or limit suckling time or frequency at the breast will not only do no good, but could do harm. However, a baby that has protracted feeds without coming off spontaneously, or a baby that feeds very frequently, may be attached to the breast incorrectly.
MANAGEMENT OF BREASTFEEDING
667
A baby that is poorly attached can also cause nipple trauma, which may give rise to engorgement and/or mastitis.
11Night feeds
The advantages of night feeds include:
- The cheeks are drawn in as the baby sucks.
Other books
Keeplock: A Novel of Crime by Stephen Solomita
Beyond the Burning Lands by John Christopher
Channel 20 Something by Amy Patrick
My Deepest Desire (Hidden Desires) by Dane, Sanya
Impervious (The Ascension Series Book 1) by Heather Letto
Maggie MacKeever by Our Tabby
The Stone Dogs by S.M. Stirling
Cyclogeography by Jon Day
Snowed In by Rachel Hawthorne