Pediatric Examination and Board Review (93 page)
Read Pediatric Examination and Board Review Online
Authors: Robert Daum,Jason Canel

(E) stool
7.
If this is infectious mononucleosis caused by Epstein-Barr virus (EBV), what is the simplest way to support the diagnosis?
(A) EBV titers
(B) CBC
(C) throat culture
(D) monospot test
(E) nasal swab
8.
If you found that this patient had EBV mononucleosis, what is your treatment?
(A) no treatment
(B) oral steroids
(C) amoxicillin
(D) ceftriaxone
(E) azithromycin
9.
Under which age does the monospot test to detect heterophil antibody decrease significantly in sensitivity?
(A) 1 year
(B) 2 years
(C) 4 years
(D) 8 years
(E) 10 years
10.
Another child who was thought to have mononucleosis had the following test results:
Immunoglobulin (Ig)G to viral capsid antigen
(VCA): positive
IgM to VCA: negative
Early antigen (EA): negative
Antibody against EBNA (EBV nuclear antigen): positive
What can be deduced from these results?
(A) no present or past EBV infection
(B) definite past infection
(C) acutely infected
(D) either past infection or recent infection
(E) none of the above
11.
How long does infection with EBV last?
(A) 1 month
(B) 6 months
(C) 1 year
(D) 2 years
(E) lifelong
12.
The most reasonable indication for treating mononucleosis with steroids is
(A) severe splenomegaly
(B) severe pain from sore throat
(C) impending airway obstruction
(D) hemolytic anemia
(E) myocarditis
13.
A patient with mononucleosis and splenomegaly should be advised to avoid contact sports for at least how long?
(A) 1-2 weeks
(B) 3 weeks-6 months
(C) 1 year
(D) life
(E) none of the above; no recommendation to avoid contact sports
14.
The 14-year-old boy from the vignette calls you 10 days after you saw him in your office and diagnosed him with mononucleosis. He now has a fever of 103.2°F (39.5°C), cannot swallow, and feels that he cannot open his mouth easily. You see him hours later in the office and you note that his voice is quite muffled. On examination, his temperature is 100.6°F (38.1°C) (he took acetaminophen 2 hours prior). The blood pressure (BP) is 110/65. He cannot open his mouth wide, but on minimal opening you note white exudates covering both tonsils, marked tonsillar enlargement, right greater than left, and a visible bulge at the superior aspect of the right tonsil. What is his diagnosis?
(A) secondary strep pharyngitis
(B) peritonsillar abscess
(C) retropharyngeal abscess
(D)
Mycoplasma pneumoniae
cellulitis
(E)
Corynebacterium diphtheriae
infection
15.
Which of the following should be part of his management?
(A) IV clindamycin
(B) surgical incision and drainage
(C) IV ampicillin
(D) tonsillectomy
(E) A, B, and D
16.
Which of the following is
not
a relative indication for tonsillectomy?
(A) more than 8 episodes of viral pharyngitis in 1 year
(B) more than 6 episodes of group A streptococcal pharyngitis in 1 year
(C) acute airway obstruction concurrent with peritonsillar abscess
(D) peritonsillar abscess following recurrent tonsillitis
(E) obstructive sleep apnea
17.
A patient’s mother is worried about the complications of tonsillectomy. Which of the following is not a known complication?
(A) velopharyngeal insufficiency
(B) hemorrhage
(C) sinusitis
(D) eustachian tube injury
(E) dehydration
18.
Adenoidectomy is potentially beneficial in all of the following except
(A) chronic recurrent sinusitis
(B) hyponasal speech
(C) hypernasal speech
(D) submucous cleft palate
(E) excessive snoring
ANSWERS
1.
(D)
The most likely diagnosis for this boy is EBV mononucleosis because of his age, presenting symptoms, and examination. Mononucleosis can present with a wide range of severity, but most patients have fever that averages 6 days’ duration, exudative pharyngitis, lymphadenopathy that is most often anterior and posterior cervical but can be generalized, fatigue, and hepatosplenomegaly in 50% of patients.
2.
(C)
Seventy-nine percent of infectious mononucleosis syndromes are caused by EBV, a herpesvirus. The other 21% are caused by CMV. Sore throat with exudative tonsillitis is more common with EBV than CMV mononucleosis; fever is a predominant feature of CMV mononucleosis. With CMV, the heterophil agglutinin test (monospot test) is negative.
3.
(C)
Pharyngoconjunctival fever is associated with adenovirus.
4.
(E)
5.
(E)
6.
(C)
Despite the physical findings of mononucleosis, often centered in the oropharynx, blood is the most useful specimen because serologic testing will produce a more timely diagnosis. Viral culture is possible by pharyngeal swab but is performed in only a few laboratories and may be positive for many years after the acute infection.
7.
(D)
The monospot test is relatively sensitive and specific in this age group. A positive test may be considered diagnostic. Even though a single EBV serology determination might give you helpful information, repeat testing for convalescent serology may be necessary, and thus this serologic approach may not be simplest. A CBC with an absolute lymphocytosis in the second week of illness is supportive of the diagnosis but not specific. A throat cultures for viral isolation does not necessarily indicate acute infection in any disease where viral persistence is common. EBV viral isolation is not routinely available.
8.
(A)
Because mononucleosis has a viral etiology (EBV), no antibacterial therapy is warranted. A high percentage of patients with mononucleosis who are exposed to ampicillin or amoxicillin develop a nonallergic morbilliform rash. Penicillin is an acceptable alternative if antibacterial therapy is indicated. About 10-30% of patients with mononucleosis are concomitantly group A strep positive; the treatment of the latter can complicate the diagnosis of the former. Steroids should only be considered in severe cases of mononucleosis.
9.
(C)
Children younger than 4 years of age may have EBV infectious mononucleosis but lack heterophil antibodies. The reason is not known. If infectious mononucleosis is suspected in these young children, EBV serology should be performed.
10.
(D)
The VCA IgM and IgG occur in high titers early after infection begins. The IgM response lasts for 3-5 months, and IgG can be detected indefinitely. The EA likewise is positive in the first 2 weeks of infection and peaks at about 3 months. It is important to note that if tested too early, the EA and the IgM VCA may not yet be positive. EBNA antibodies are not present until several weeks to months after onset of infection. So although a positive EBNA result excludes acute infection, it cannot differentiate between recent or past infection.
11.
(E)
EBV, like other herpesviruses, establishes lifelong latent infection. As opposed to the other herpesviruses, reinfection with EBV is usually asymptomatic.
12.
(C)
There are few objective data that document the effectiveness of corticosteroids in infectious mononucleosis. Many clinicians use them in the management of impending or actual airway obstructions. They should otherwise be avoided as unnecessary therapy that may even increase the rate of occurrence of certain complications like encephalitis. Severe pain may be treated adequately with other medications.
13.
(B)
Splenic enlargement is common in mononucleosis, but splenic rupture is rare (0.1-0.2%). Rupture most commonly occurs within the first 3 weeks following diagnosis. Athletes are sometimes counseled to wait up to 6 months before resuming contact sports. At the time of activity resumption, neither the spleen nor the liver should be enlarged.
14.
(B)
Although a peritonsillar abscess is most often a complication of group A streptococcal pharyngitis, EBV infectious mononucleosis and group A streptococci are commonly present simultaneously. This patient has fever, trismus, and an obvious tonsillar bulge, the triad of which strongly suggests the diagnosis.
15.
(E)
In addition to standard treatment of peritonsillar abscess, parenteral antibiotics, and surgical drainage, this patient is a candidate for tonsillectomy because of his history of recurrent tonsillitis. This would be performed after the acute episode resolves. Ampicillin is an unwise choice because of the known increase in the incidence of rash when patients with mononucleosis are given ampicillin or derivatives. This rash does not represent ampicillin allergy. It presents as a maculopapular pruritic confluent rash mainly over the trunk and includes the palms and soles (see
Figure 57-1
).
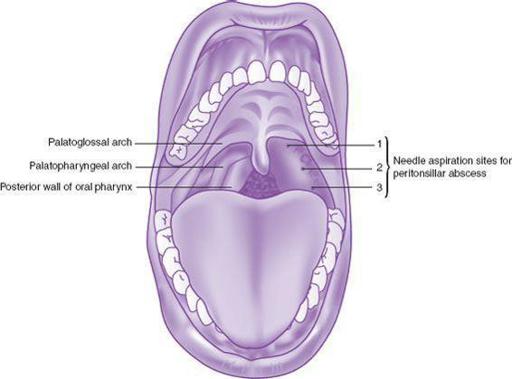
FIGURE 57-1.
When needle aspiration is used to manage peritonsillar abscess, aspiration should be attempted at each of these three anatomic locations. (Reproduced, with permission, from Stone CK, Humphries RL. Current Diagnosis & Treatment: Emergency Medicine, 6th ed. New York: McGraw-Hill, 2008. Fig. 30-9.)
16.
(A)
Viral pharyngitis is never an indication for tonsillectomy. Repeated bacterial infection of the tonsils may be, although the number of infections per year that warrant tonsillectomy is controversial. Some recommend it when there are more than 3 episodes per year, others wait for more than 6 per year, and yet others await more than 3 episodes a year for 3 consecutive years. Other reasons for performing tonsillectomy are obstructive sleep apnea or, rarely, acute airway obstruction.