Pediatric Primary Care Case Studies (85 page)
Read Pediatric Primary Care Case Studies Online
Authors: Catherine E. Burns,Beth Richardson,Cpnp Rn Dns Beth Richardson,Margaret Brady
Tags: #Medical, #Health Care Delivery, #Nursing, #Pediatric & Neonatal, #Pediatrics

Bilateral conjunctival injection with watery discharge and itching rather than pain characterizes allergic conjunctivitis. It also may be associated with allergic rhinitis. Often there is a seasonal pattern, most commonly in the spring, summer, and fall with recurrence each year. Vernal conjunctivitis may develop due to severe allergic conjunctivitis. Patients will have cobblestoning on the upper tarsal plate due to giant papillae. This most commonly occurs in prepubertal children and boys more often than girls (Gigliotti, 1995).
Ocular foreign body is commonly characterized by unilateral conjunctival injection, watery discharge, and a foreign body sensation. Chemical conjunctivitis results when an irritating substance comes in contact with the conjunctiva. Common agents include silver nitrate used in newborns for prophylaxis of ophthalmia neonatorium, household cleaners, pesticides, and smoke (Olitsky et al., 2007).
Patients with periorbital and orbital cellulitis will have conjunctival injection as well. However, in both of these infections, patients will have significant unilateral eyelid edema, erythema, and chemosis or swelling of the bulbar conjunctiva. Often they are unable to open the eyelid due to swelling. They may have fever and will often appear ill with orbital cellulitis as well as have proptosis of the affected eye, pain with movement of the eye, impaired eye movement, and visual impairment (Wald, 2004).
Keratitis and uveitis are often associated with a red eye. Patients with keratitis may present with intense pain, photophobia, and corneal clouding. Patients may have a history of contact lens use. Herpes simplex virus can cause keratitis, as can
S. pneumoniae, S. aureus
, and
Pseudomonas.
Uveitis in children is often due to a systemic illness such as juvenile idiopathic arthritis, inflammatory bowel disease, lupus, Kawasaki disease, or Stevens-Johnson syndrome. Patients often complain of pain, vision loss, and photophobia in addition to conjunctival injection (Gigliotti, 1995). Kawasaki disease is characteristically associated with a bilateral bulbar, nonpurulent conjunctivitis, fever for 5 days or longer, rash, oral mucosal involvement, swelling of hands and feet, and lymphadenopathy (Pickering et al., 2006). In addition to widespread vesicles and bullae of the face, trunk, and extremities, patients with Stevens-Johnson syndrome often have eye involvement characterized by uveitis and corneal abrasion as well as oral mucosal involvement. Glaucoma may present with a red eye, corneal clouding, and pain; however, outside of the neonatal period, it is not a common disorder in children (Gigliotti).
Management
Do you need to do anything to confirm the diagnosis, such as laboratory studies?

Laboratory studies usually are not needed to confirm the diagnosis of bacterial conjunctivitis. Culture of the eye drainage may be obtained, but patients are usually treated presumptively based on the history and physical examination findings, which suggest bacterial conjunctivitis. In neonates, bacterial culture may be warranted because
N. gonorrhoea
or
C. trachomatis
require systemic treatment, not just topical treatment.
Therapeutic plan: What will you do therapeutically?
The plan is determined by the type of conjunctivitis the patient has. Different treatments exist for the various causes of conjunctivitis.
Treatment Options
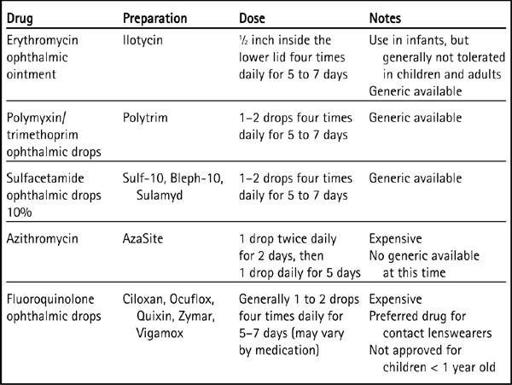
Bacterial, viral, and allergic conjunctivitis are all generally self-limited illnesses. Treatment of bacterial conjunctivitis has some advantages because it will decrease the length of illness, possibly prevent the spread of the bacteria, and decrease the risk of complications. In addition, children are usually not allowed to return to the daycare or school setting unless treatment has been initiated. The mainstay of treatment of bacterial conjunctivitis is topical antibiotics. Because a culture is not usually obtained, a broad-spectrum topical antibiotic is usually the choice for treatment (Hwang, Schanzlin, Rotberg, Foulks, & Raizman, 2003). Topical antibiotics can be either drops or ointment, with ointment commonly used for infants. Typically older children do not tolerate ointment as well because it can cause distorted vision. Common antibiotics prescribed include erythromycin ointment, trimethoprim sulfate/polymyxin drops, or sulfacetamide drops. Fluoroquinolone drops and azithromycin drops are also used but may promote resistance and are generally more expensive than the other choices because they are relatively newer preparations. (See
Table 21-2
.) In cases of ophthalmia neonatorum, systemic treatment with intravenous antibiotics is required. In children who present with conjunctivitis with ipsilateral otitis media, oral antibiotics should be used such as amoxicillin/clavulanate. Patients who wear contact lenses need to be instructed to refrain from wearing their contacts until the conjunctivitis has resolved. If the lenses are disposable, they should be discarded along with the lens case (Olitsky et al., 2007).
Viral conjunctivitis does not generally require any treatment. The symptoms may last for up to 2 to 3 weeks. The emphasis should be placed on prevention of the spread of viral conjunctivitis. In cases of adenoviral conjunctivitis associated with swimming pools, adequate chlorination of the water will prevent the spread of adenovirus (Gigliotti, 1995).
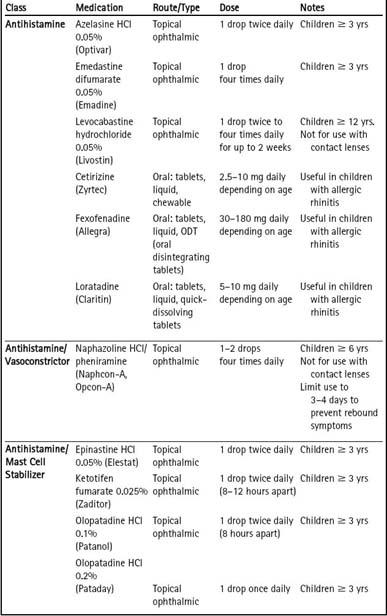
Treatment of allergic conjunctivitis should include avoidance of the inciting allergen; however, this may be difficult to do because many allergens are pervasive and difficult for patients to avoid. Cold compresses and lubricating eye drops can also provide relief. Patients can use either topical or oral preparations to help manage allergic conjunctivitis. In cases when allergic conjunctivitis is present in combination with allergic rhinitis, patients will benefit from oral, nonsedating antihistamines such as cetirizine, loratadine, or fexofenadine. Topical ophthalmic medications include antihistamines, antihistamines and mast cell blockers, decongestants, and corticosteroids. Decongestants are not recommended because although they may reduce symptoms, they do not help stop the allergic reaction. Repeated use of these can cause a rebound conjunctival injection or conjunctivitis medicamentosa. The combination of an antihistamine and mast cell blocker
offers quick relief of the symptoms and helps stop the allergic reaction. Examples of this are epinastine hydrochloride 0.05%, ketotifen fumarate 0.025%, or olopatadine hydrochloride 0.1%. These medications are given twice daily, but sometimes cause burning. Refrigerating the medications can sometimes decrease the burning sensation. Corticosteroids should be used only in consultation with an ophthalmologist (Boguniewicz & Leung, 2007; Ono & Abelson, 2005).
Table 21–2 Topical Antibiotics for Bacterial Conjunctivitis
Both chemical conjunctivitis and ocular foreign body require removal of the offending agent. Immediate irrigation of the eye with profuse amounts of water is necessary to help prevent the effects of chemical exposure of the eye. Conjunctival injection, edema, and irritation may persist even if the chemical or foreign body is removed. Consultation with an ophthalmologist may be necessary in certain cases of chemical exposure and foreign body.
Both periorbital and orbital cellulitis require treatment with systemic antibiotics and may require hospitalization. Orbital cellulitis requires intravenous antibiotics, and an ophthalmologist should be consulted to help manage the patient because surgery may be required (Wald, 2004). In patients with suspected uveitis and keratitis, referral to an ophthalmologist for evaluation and management is required.
The summary of treatments of different types of conjunctivitis is found in
Table 21-3
.
Table 21–3 Treatments for Allergic Conjunctivitis
In Jack’s case, you decide to prescribe trimethoprim/polymyxin drops. His mother is instructed to instill two drops into the affected eye four times daily for 7 days.
Educational plan: What will you do to educate Jack and his mother about bacterial conjunctivitis and its management?
Points to make through discussion:
Explain the diagnosis of bacterial conjunctivitis.