Pocket Medicine: The Massachusetts General Hospital Handbook of Internal Medicine (66 page)
Read Pocket Medicine: The Massachusetts General Hospital Handbook of Internal Medicine Online
Authors: Marc Sabatine
Tags: #Medical, #Internal Medicine

BOOK: Pocket Medicine: The Massachusetts General Hospital Handbook of Internal Medicine
2.13Mb size Format: txt, pdf, ePub
thrombosis (HIT): screen for DVT; unclear duration of subsequent anticoag (until plt count recovers, often ~2–3 mo if no clot);
25–50% thrombosis rate w/in 30 d
• Heparin use if h/o HIT: if PF4 Ab
Hemolytic-uremic syndrome (HUS) & thrombotic thrombocytopenic purpura (TTP)
• Definition: vascular occlusive disorders w/ systemic (TTP) or intrarenal (HUS) plt aggreg.
→ thrombocytopenia & mechanical injury to RBCs (MAHA) (
NEJM
2002;347:589)
HUS triad
= thrombocytopenia + MAHA + renal failure
TTP pentad
(all 5 in only ~5%) = thrombocytopenia + MAHA (100%) ± Δ MS (65%) ± renal failure (50%) ± fever (25%)
• Pathophysiology: mechanism in most HUS cases is distinct from TTP (
NEJM
1998;339:1578)
HUS
: Shiga toxin binds & activates renal endothelial cells & plts → intrarenal thrombi
TTP
: ↓ ADAMTS13 protease activity
or
inhibitor→ persistence of large vWF multimers on endothelial surface → adhesion and aggregation of passing platelets → thrombosis
• Clinical manifestations and associations
HUS
: usually in children; prodrome of bloody diarrhea due to enterohemorrhagic
E. coli
TTP
: usually in adults;
idiopathic, drugs
(CsA, tacrolimus, gemcitabine, mitomycin-C, ticlopidine, clopidogrel, quinine), HIV, pregnancy, HSCT, autoimmune disease, familial
• Dx: unexplained
thrombocytopenia
(typically <20k) +
MAHA
→
sufficient for dxschistocytes
(>2–3/hpf),
Biopsy: arterioles filled with platelet hyaline thrombi
Ddx: DIC, vasculitis, malignant hypertension, preeclampsia/HELLP syndrome
• Treatment:
urgent plasma exchange
± glucocorticoids if suspected; FFP if delay to plasma exchange (
Blood
2010;116:4060); ? eculizumab in HUS (
NEJM
2011;364:2561);
plt transfusions contraindicated
→ ↑ microvascular thrombosis (
NEJM
2006;354:1927)
Disseminated intravascular coagulation (DIC):
see “Coagulopathies”
DISORDERS OF PLATELET FUNCTION
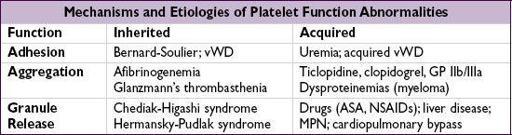
Tests of platelet function
• Bleeding time: global screen of platelet function;
not reliable and rarely used
• Platelet aggregation tests: measure aggregation in response to agonists (eg, ADP)
von Willebrand’s disease (vWD)
(
NEJM
2004;351:683 & 2012;367:1954)
• von Willebrand’s factor (vWF) function = platelet glue & plasma carrier of factor VIII • vWD most common inherited (usually auto dom) bleeding disorder;
85% (type 1) have partial quantitative defic of vWF,
15% (type 2) have qualitative defic in vWF
• Acquired vWD: a/w many disorders (malig, MPN w/ ↑ plt count; autoimmune; hypo-thyroidism; drugs) and caused by different mechanisms (anti-vWF Abs, ↑ clearance, ↓ synthesis); Heyde’s syndrome = vWF destruction by severe AS, a/w GI AVMs/bleed • Diagnosis: ↓
vWF:Ag
, ↓
vWF activity
(measured by ristocetin cofactor assay), ↓
factor VIII
, ± ↑ PTT, ± ↓ platelets; confirm with
vWF multimer analysis
• Clinical condition, factor VIII levels and ristocetin cofactor assay useful to guide Rx decision • Rx:
desmopressin
(dDAVP, IV/IN) → ↑ endothelial cell release of vWF; efficacy depends on type (avoid in Type 2), ∴ ✓ response before use w/ subseq. bleeding or procedures;
vWF replacement
: cryoprecipitate, factor VIII concentrates rich in vWF, recomb. vWF
Uremic bleeding
• Uremia → platelet dysfunction including ↓ aggregation, impaired adhesiveness • Treatment:
dDAVP
, cryoprecipitate, correct anemia (improves plt aggregation and
adhesion by increasing plt interactions with endothelium), consider holding anti-plt agents
COAGULOPATHIES

Further coagulation tests
• Mixing study: useful if ↑ PT or PTT; mix Pt’s plasma 1:1 w/ normal plasma and retest PT/PTT normalizes → factor
deficiency
; PT/PTT remains elevated → factor
inhibitor
• Coagulation factor levels: useful if mixing study suggests factor deficiency
DIC → all factors consumed; ∴ ↓ factors V and VIII liver disease → ↓ all factors
except
VIII; ∴↓ factor V, normal factor VIII vitamin K deficiency → ↓ factors II, VII, IX, X (and protein C, S); ∴ normal V and VIII
•
DIC screen
: fibrinogen (consumed), fibrin degradation products (FDPs,
Hemophilias
(
NEJM
2001;344:1773)
• X-linked recessive
factor VIII
(hemophilia A) or
factor IX
(hemophilia B)
deficiency
• Classification: mild (5–25% normal factor activity), moderate (1–5%) or severe (<1%) • Clinical manifestations: hematomas, hemarthroses, bruising, bleeding (mucosal, GI, GU) • Diagnosis: ↑ PTT (normalizes w/mixing study), normal PT & vWF, ↓ factor VIII or IX
• Treatment: purified/recomb. factor VIII or IX concentrate, desmopressin (mild disease), aminocaproic acid; recomb. factor VIIa if factor inhib., cryo (only has factor VIII)
Coagulation factor inhibitors
• Etiologies: hemophilia (treated with factor replacement); postpartum; lymphoproliferative disorders and other malignancies; autoimmune diseases; most commonly anti–factor VIII • Diagnosis: ↑ PTT (does
not
normalize w/mixing study); Bethesda assay quantitates titer • Treatment: high titer →
recomb. factor VIIa
, porcine factor concentrates, activated prothrombin complex; others → high-purity human factor, plasmapheresis, immunosupp. w/ steroids, cyclophosphamide and/or rituximab (
Curr Opin Hematol
2008;15:451)
Disseminated intravascular coagulation (DIC)
(
NEJM
1999;341:586)
• Etiologies: trauma, shock, infection, malignancy (esp. APL), obstetric complications • Pathogenesis:
massive
activation of coagulation that overwhelms control mechanisms
thrombosis
in microvasculature → ischemia + microangiopathic hemolytic anemia acute consumption of coagulation factors and platelets →
bleeding
chronic DIC → able to replete factors and platelets →
thrombosis
• Diagnosis: ↑ PT, ↑ PTT, ↓
fibrinogen
(may be
nl
b/c acute phase),
/
D-dimer
, ↓ plts,
chronic
DIC:
FFP
,
cryoprecipitate
(goal fibrinogen
Other books
The Navigator by Clive Cussler, Paul Kemprecos
The Lady And The Lake by Collier, Diane
What Happens After Dark by Jasmine Haynes
The I.P.O. by Dan Koontz
The French Code by Deborah Abela
Koko the Mighty by Kieran Shea
The Road to Gretna by Carola Dunn
Adobe Flats by Colin Campbell
New World Order (War of the Fae: Book 4) by Casey, Elle
My Sweet Valentine by Dairenna VonRavenstone