Resident Readiness General Surgery (32 page)
Read Resident Readiness General Surgery Online
Authors: Debra Klamen,Brian George,Alden Harken,Debra Darosa
Tags: #Medical, #Surgery, #General, #Test Preparation & Review

4.
In order to minimize the use (and consequently the risk) of opiates, adjunct analgesic medications are sometimes used. The 2 most common medications are NSAIDs and acetaminophen (Tylenol). These are most effective if written “around the clock,” that is, they can serve as basal pain control while the opiates can be used for breakthrough pain. Numerous studies have demonstrated that this type of regimen results in lower total usage of opiates.
Acetaminophen is most useful after the patient is eating, although there is a formulation that can be given per rectum (PR) if the patient tolerates this route of administration. An intravenous formulation of acetaminophen (trade name Ofirmev) was recently approved by the FDA for postoperative pain management. However, as this is a relatively new medication prevalence of usage varies between institutions, and you should check with your senior resident or attending before ordering it. Acetaminophen is usually well tolerated, although it does have the well-known risk of hepatotoxicity. Total acetaminophen dose should not exceed 4 g in 24 hours—remember that this total includes any acetaminophen given as part of a mixed formulation such as Percocet or Vicodin. Acetaminophen should also be minimized in those patients with existing hepatic disease or those who have just undergone a liver operation.
Like acetaminophen, NSAIDs are also commonly added to a patient’s medical regimen in order to minimize opiate usage. The only commonly used IV NSAID is ketorolac (trade name Toradol), which is dosed at 15 or 30 mg IV q6h. As discussed above, it is usually ordered in a scheduled (rather than prn) fashion. While effective, Toradol does, however, have several important side effects. Toradol (as well as the other NSAIDs) is a mild anticoagulant, and for this reason you should never initiate its use postoperatively without first discussing it with the senior resident or attending. Second, NSAIDs can reduce renal perfusion and should be avoided in patients with impaired renal function. Patients on Toradol should have a daily chemistry ordered to check for an increase in their creatinine levels. NSAIDs also inhibit bone growth and are generally avoided in patients with fractures.
5.
Generally, patients should be transitioned to an oral pain regimen as soon as they are started on a diet. Some surgeons will start their patients on PO pain medication when they are advanced to liquids; however, others will wait until patients are taking a regular diet, so you should always check before making this change. The most commonly used postoperative oral pain medications are combinations of acetaminophen and an opioid. These include Percocet (acetaminophen and oxycodone), Vicodin (acetaminophen and hydrocodone), and Tylenol #3 (acetaminophen and codeine). Morphine and Dilaudid can also be prescribed in oral form, but these are generally reserved for patients with chronic opioid usage (and thus tolerance) and are not used in standard postoperative situations. Oral NSAIDs, most commonly ibuprofen at 400 mg PO q6h, can be given in addition to the above medications, again in an effort to reduce the total opioid usage.
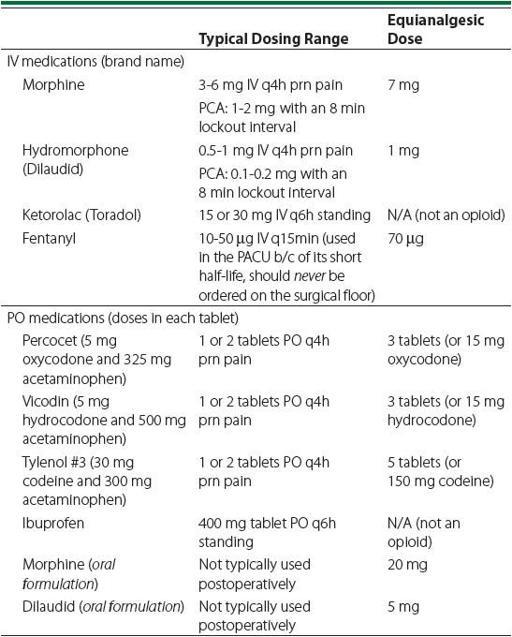
All opioids have different analgesic strengths per milligram and you should be generally familiar with the conversion factors between them.
Table 23-1
shows a chart of standard pain medication doses and their relative strengths.
Table 23-1
.
Standard Pain Medications and Their Relative Strengths
Although oral opioids have less severe side effects than those given IV, they still cause constipation. Patients should be placed on a bowel regimen when receiving them and be given a prescription for Colace (or another stool softener) on discharge.
TIPS TO REMEMBER
Assume that patients with an unusually high level of pain after an operation have a surgical complication. Inadequate analgesia is a diagnosis of exclusion.
COMPREHENSION QUESTIONS
1.
In which of the following patient populations should ketorolac (brand name Toradol)
not
be used? (Choose all that apply.)
A. Trauma patients with subdural hematomas
B. Patients with type II diabetes
C. Patients with chronic renal insufficiency
D. Patients with dementia
2.
Which of the following is an appropriate PCA order for a patient immediately after a laparotomy?
A. Morphine 3 mg per dose, with a lockout interval of 2 minutes
B. Dilaudid 1 mg per dose, with a lockout interval of 8 minutes
C. Morphine 1 mg per dose, with a lockout interval of 8 minutes
D. Dilaudid 0.2 mg per dose, with a lockout interval of 2 minutes
3.
On postoperative day 1 after a laparoscopic gastric bypass, a patient is complaining of what you think is unusually intense epigastric pain. What other finding would make you most concerned for an anastomotic leak?
A. Heart rate of 120
B. White blood cell (WBC) count of 10.5
C. Urine output of 75 mL/h
D. Blood pressure of 160/80
4.
What dose of Dilaudid IV is equivalent to the amount of oxycodone in a single Percocet tablet?
A. 0.1 mg
B. 0.33 mg
C. 0.5 mg
D. 1 mg
Answers
1.
Both A and C
. Toradol is an anticoagulant and can be nephrotoxic, so it should be avoided in patients with (or at risk for) bleeding or impaired renal function.
2.
C
. All of the other choices have either too high a dose (morphine 3 mg or Dilaudid 1 mg) or too short a lockout interval (2 minutes).
3.
A
. Tachycardia along with an abnormal amount of pain should alert you that a complication may have occurred.
4.
B
. Each Percocet tablet contains 5 mg of oxycodone, which is equivalent to 0.33 mg of IV Dilaudid.
 A 72-year-old Man With Acute Confusion Postoperatively
A 72-year-old Man With Acute Confusion Postoperatively
Other books
People of the Deer by Farley Mowat
Night of a Thousand Stars by Deanna Raybourn
After Midnight by Nielsen, Helen
A Prisoner in Malta by Phillip Depoy
Jar City by Arnaldur Indridason
Richardson Scores Again by Basil Thomson
Hold Hands in the Dark by Katherine Pathak
Arrested Love by Jean Baker
Longarm on the Overland Trail by Tabor Evans
Wreckers or Checkers: In It to Win It by H. M. Montes