Ross & Wilson Anatomy and Physiology in Health and Illness (104 page)
Read Ross & Wilson Anatomy and Physiology in Health and Illness Online
Authors: Anne Waugh,Allison Grant
Tags: #Medical, #Nursing, #General, #Anatomy

Learning outcome
After studying this section you should be able to:
explain how the diseases in this section are related to abnormal secretion of parathyroid hormone.

Hyperparathyroidism
Excess secretion of parathyroid hormone (PTH), usually by benign tumours of a gland, causes release of calcium from bones, raising blood calcium levels (hypercalcaemia). The effects may include:
•
polyuria and polydipsia
•
formation of renal calculi
•
anorexia and constipation
•
muscle weakness
•
general fatigue.
Hypoparathyroidism
Parathyroid hormone (PTH) deficiency causes hypocalcaemia, i.e. abnormally low blood calcium levels, and is much less common than hyperparathyroidism. There is reduced absorption of calcium from the small intestine and less reabsorption from bones and glomerular filtrate. Low blood calcium causes:
•
tetany
(
Fig. 9.17
)
•
psychiatric disturbances
•
paraesthesia
•
grand mal seizures
•
in some cases, cataracts (opacity of the lens) and brittle nails.
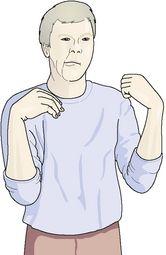
Figure 9.17
Characteristic positions adopted during tetanic spasms.
The causes of hypoparathyroidism include: damage to or removal of the glands during thyroidectomy, ionising radiation, development of autoantibodies to PTH and parathyroid cells, and congenital abnormality of the glands.
Tetany
This is caused by hypocalcaemia, because low blood calcium levels increase excitability of peripheral nerves. There are very strong painful spasms of skeletal muscles, causing characteristic bending inwards of the hands, forearms and feet (
Fig. 9.17
). In children there may be laryngeal spasm and seizures.
Hypocalcaemia
This is associated with:
•
hypoparathyroidism
•
deficiency of vitamin D or dietary deficiency of calcium
•
chronic renal failure when there is excretion of excess calcium in the urine
•
alkalosis; metabolic due to persistent vomiting, ingestion of excess alkaline medicines to alleviate indigestion, or respiratory due to hyperventilation
•
acute pancreatitis.
Disorders of the adrenal cortex
Learning outcomes
After studying this section you should be able to:
Hypersecretion of glucocorticoids (Cushing’s syndrome)
Cortisol is the main glucocorticoid hormone secreted by the adrenal cortex. Causes of hypersecretion include:
•
hormone-secreting adrenal tumours that may be benign or malignant
•
hypersecretion of adrenocorticotrophic hormone (ACTH) by the anterior pituitary
•
abnormal secretion of ACTH by a non-pituitary tumour, e.g. bronchial or pancreatic tumour
•
prolonged therapeutic use of ACTH or glucocorticoids, e.g. prednisolone, in high doses.
Hypersecretion of cortisol exaggerates its physiological effects (
Fig. 9.18
). These include:
•
painful adiposity of the face (
moon face
), neck and abdomen
•
excess protein breakdown, causing thinning of subcutaneous tissue and muscle wasting, especially of the limbs
•
diminished protein synthesis
•
suppression of growth hormone preventing normal growth in children
•
osteoporosis (
p. 421
), and kyphosis if vertebral bodies are involved
•
pathological fractures because of calcium loss from bones
•
excessive gluconeogenesis resulting in hyperglycaemia and glycosuria which can precipitate diabetes mellitus (
p. 227
)
•
atrophy of lymphoid tissue and depression of the immune response
•
susceptibility to infection due to reduced febrile response, depressed immune response and phagocytosis, impaired migration of phagocytes
•
impaired collagen production, leading to capillary fragility, cataract and striae
•
insomnia, excitability, euphoria, psychosis, depression
•
hypertension due to salt and water retention
•
menstrual disturbances
•
formation of renal calculi
•
peptic ulceration.
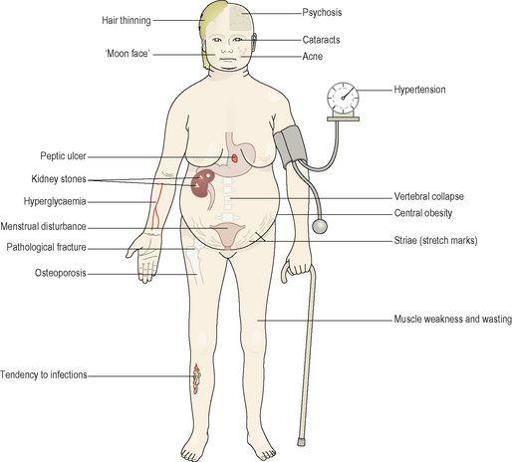
Figure 9.18
The systemic features of Cushing’s syndrome.
Hyposecretion of glucocorticoids
Inadequate secretion of cortisol causes diminished gluconeogenesis, low blood glucose levels, muscle weakness and pallor. It may be primary, i.e. due to disease of the adrenal cortex, or secondary due to deficiency of ACTH from the anterior pituitary. In primary deficiency there is also hyposecretion of aldosterone (see below) but in secondary deficiency, aldosterone secretion is not usually affected because aldosterone release is controlled by the renin–angiotensin–aldosterone system (
p. 216
).
Hypersecretion of mineralocorticoids
Excess aldosterone affects kidney function, with consequences elsewhere:
•
excessive reabsorption of sodium chloride and water, causing increased blood volume and hypertension
•
excessive excretion of potassium, causing
hypokalaemia
, which leads to cardiac arrhythmias, alkalosis, syncope and muscle weakness.
Primary hyperaldosteronism (Conn’s syndrome)
This is due to an excessive secretion of mineralocorticoids, independent of the renin–angiotensin–aldosterone system. It is usually caused by a tumour affecting only one adrenal gland.
Secondary hyperaldosteronism