Ross & Wilson Anatomy and Physiology in Health and Illness (50 page)
Read Ross & Wilson Anatomy and Physiology in Health and Illness Online
Authors: Anne Waugh,Allison Grant
Tags: #Medical, #Nursing, #General, #Anatomy

Figure 5.53
A.
Fetal circulation before birth.
B.
Changes to the fetal circulation at birth.
Ductus arteriosus
This small vessel connects the pulmonary artery to the descending thoracic aorta and diverts more blood into the systemic circulation, meaning that very little blood passes through the fetal lungs (see
Fig. 5.63
).
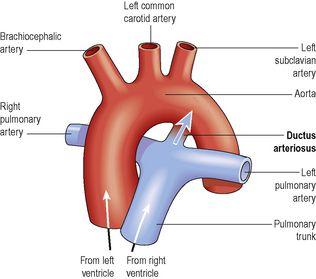
Figure 5.63
The ductus arteriosus in the fetus.
The arrow indicates the direction of flow of blood from the pulmonary circulation into the aorta.
Foramen ovale
This forms a valve-like opening (see
Fig. 5.64
) allowing blood to flow between the right and left atria, so that most blood bypasses the non-functional fetal lungs.
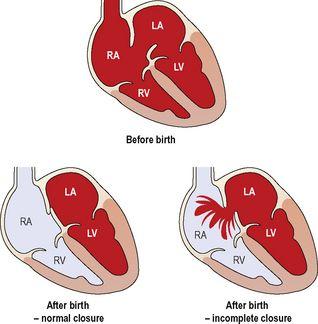
Figure 5.64
Atrioseptal valve:
normal and incomplete closure after birth.
Changes at birth (
Fig. 5.53B
)
When the baby takes its first breath the lungs inflate for the first time, increasing pulmonary blood flow. Blood returning from the lungs increases the pressure in the left atrium, closing the flap over the foramen ovale and preventing blood flow between the atria. Blood entering the right atrium is therefore diverted into the right ventricle and into the pulmonary circulation through the pulmonary veins. As the pulmonary circulation is established (see
Fig. 5.1
) blood oxygen levels increase, causing constriction and closure of the ductus arteriosus. If these adaptations do not take place after birth, they become evident as congenital abnormalities (see
Figs 5.63
and
5.64
). When the placental circulation ceases, soon after birth, the umbilical vein, ductus venosus and umbilical arteries collapse, as they are no longer required.
Shock

Learning outcomes
After studying this section, you should be able to:
define the term shock
Shock (circulatory failure) occurs when the metabolic needs of cells are not being met because of inadequate blood flow. In effect, there is a reduction in circulating blood volume, in blood pressure and in cardiac output. This causes tissue hypoxia, an inadequate supply of nutrients and the accumulation of waste products. A number of different types of shock are described.
Hypovolaemic shock
This occurs when the blood volume is reduced by 15 to 25%. Cardiac output may fall because of low blood volume and hence low venous return, as a result of different situations:
•
severe haemorrhage – whole blood is lost
•
extensive burns – serum is lost
•
severe vomiting and diarrhoea – water and electrolytes are lost.
Cardiogenic shock
This occurs in acute heart disease when the damaged heart muscle cannot maintain an adequate cardiac output, e.g. in myocardial infarction.
Septic shock (bacteraemic, endotoxic)
This is caused by severe infections in which bacterial toxins are released into the circulation. These toxins trigger a massive inflammatory and immune response, and many powerful mediators are released. Because the response is not controlled, it can cause multiple organ damage, including hypotension because of widespread vasodilation, depression of myocardial contractility, poor tissue perfusion and tissue death (necrosis).
Neurogenic shock
The causes include sudden acute pain, severe emotional experience, spinal anaesthesia and spinal cord damage. These interfere with normal nervous control of blood vessel diameter, leading to hypotension.
Anaphylactic shock
Anaphylaxis is a severe allergic response that may be triggered in sensitive individuals by substances like penicillin, peanuts or latex rubber. Vasodilation, provoked by systemic release of mediators, e.g. histamine and bradykinin, causes venous pooling and hypotension. Severe bronchoconstriction leads to respiratory difficulty and hypoxia. Onset is usually sudden, and in severe cases can cause death in a matter of minutes if untreated.
Physiological changes during shock
In the short term, these are associated with physiological attempts to restore an adequate blood circulation –
compensated shock
(
Fig. 5.54
). If the state of shock persists, the longer-term changes may be irreversible.
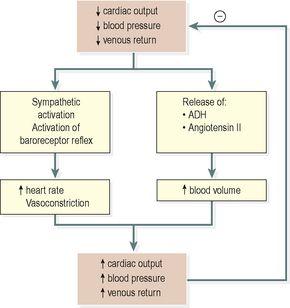
Figure 5.54
Compensatory mechanisms in shock.
Compensated shock
As the blood pressure falls, a number of reflexes are stimulated and hormone secretions increased in an attempt to restore it. These raise blood pressure by increasing peripheral resistance, blood volume and cardiac output (
Fig. 5.54
).
Increased sympathetic stimulation increases heart rate and cardiac output, and also causes vasoconstriction, all of which increase blood pressure. Low blood volume and increased osmolarity of the blood cause secretion of ADH (
p. 213
) and activation of the renin–angiotensin–aldosterone system (
p. 338
). Consequent release of aldosterone reduces water and sodium excretion and promotes vasoconstriction. The veins also constrict, helping to reduce venous pooling and support venous return.
If these compensatory mechanisms, plus any medical interventions available, are sufficient, then perfusion of the heart and brain can be maintained, and the patient’s condition may be stabilised.
Uncompensated shock
If the insult is more severe, shock becomes a self-perpetuating sequence of deteriorating cardiovascular function –
uncompensated shock
(
Fig. 5.55
). Hypoxia causes cellular metabolism to switch to anaerobic pathways (
p. 308
), resulting in accumulation of lactic acid and progressive acidosis, which damages capillaries. The capillaries then become more permeable, leaking fluid from the vascular system into the tissues, further lowering blood pressure and tissue perfusion. Also, the accumulation of waste products causes vasodilation, making it harder for control mechanisms to support blood pressure. Organs, including the heart, are deprived of oxygen and may start to fail.