Examination Medicine: A Guide to Physician Training (7 page)
Read Examination Medicine: A Guide to Physician Training Online
Authors: Nicholas J. Talley,Simon O’connor
Tags: #Medical, #Internal Medicine, #Diagnosis

Practice for the short cases is also important. More examinees used to fail these than the long cases, although this has changed now that the long cases are receiving more emphasis. It is valuable to have senior colleagues, as well as peers, take you on short cases. Travelling to other hospitals to practise is also worthwhile, because you have to examine patients in strange surroundings while being watched by unfamiliar examiners. It also relieves the boredom somewhat. The best practice examiner is the one who frightens candidates a little but does not demolish them when they make an error. Seek out constructive criticism. For example, many candidates practise in pairs, with each person taking turns to be the examiner. Practising being an examiner helps you to appreciate the bad habits that annoy the real examiners.
Equipment is always provided at the hospital where the examination is held. However, it is important to take the following:
•
a familiar stethoscope that you have used for a long time. Do not buy a new fancier stethoscope the day before the test; it takes time to get used to a new instrument. Electronic stethoscopes are not generally allowed unless a candidate has a hearing problem and has obtained permission from the College
•
a hand-held eye card – obtainable from OPSM for a moderate charge and essential for cranial nerve or eye examinations (see Ch 16)
•
a red-tipped hatpin – you can buy a plain one and paint the top with nail polish; this is invaluable for visual field testing (see Ch 16)
•
paper and pens.
It is debatable whether candidates should take in their own bags of instruments. Many favour bringing their own ophthalmoscope and pocket torch (with fresh or recharged batteries in both). Others also like to have cotton wool, neurology pins (an unused one for each case) and spatulas, as well as tuning forks (256 Hz and 128 Hz) and a patella hammer, which is too much to carry in the pockets. This has led to a trend for leather briefcases to house all the equipment (see
Fig 3.3
). However, the occasional difficult examiner has been known to complain about this! There is a legend about one candidate’s
briefcase, which was filled with such elaborate equipment, including an inverted cardigan for testing dressing apraxia, that his examiners spent their time inspecting the contents rather than watching him examine the patient (not a recommended approach!).
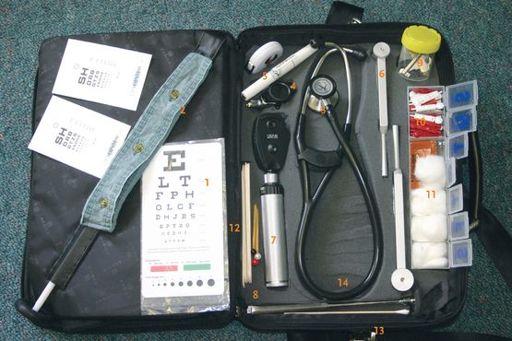
FIGURE 3.3
A candidate’s bag
1.
Eye charts
2.
Buttons and long patella hammer (underneath)
3.
Stethoscope
4.
Torch
5.
Tape measure
6.
Tuning forks
7.
Ophthalmoscope and auriscope
8.
Hatpins (red and white)
9.
Jar with lid (containing key for key grip assessment)
10.
Disposable neurology pins
11.
Cotton wool
12.
Spatula
13.
Cotton buds and spare patella hammer
14.
Carefully shaped foam inserts
A few more cautionary tales:
•
Candidates who have just bought their bags have been known to forget the combination number needed to release the lock at the critical moment in the exam when the bag has to be opened.
•
One candidate placed her open bag on the sink in the examination room for her first case, only to have the bag flooded with water when one of the examiners leaned closer to watch the examination and accidentally turned on the tap above the sink (
Fig 3.4
).

FIGURE 3.4
Incorrect positioning of bag #1
•
Leaving your bag on the floor might also be problematic. Many a examiner has been anxious that a candidate might walk backwards, trip over his or her bag and be impaled by a patella hammer (
Fig 3.5
).

FIGURE 3.5
Incorrect positioning of bag #2
•
During the assessment of the patient by the examiners one examiner mocked the old-fashioned stethoscope of his colleague: ‘You have a 19th-century stethoscope and I have a 21st-century one,’ he said. On going to examine the patient with his electronic stethoscope (not usually allowed to candidates), he stopped and said; ‘Ah, the battery is flat.’ ‘Don’t worry, you can borrow mine,’ said his helpful colleague. If you have permission to use one make sure it is charged. It would be embarrassing to have to ask to borrow the examiner’s.
•
Most candidates fly in to the examination city on the day before their exam. At least one candidate arriving in jeans and a T-shirt found that his luggage, containing his suit and tie, had been sent by the airline to Hawaii (or somewhere). It was too late to buy more clothes. He sat the exam in these casual clothes, having explained to the exam organisers what had happened. The story had a happy ending, but the anxiety caused by such an occurrence is probably best avoided. Carry your exam clothes onto the aeroplane with you. Check, however, that there is nothing in your exam bag that will disturb the airport security people. They are easily alarmed.
•
It is important that clothing used in the exam fits properly. The examiners were alarmed to see a candidate whose suit was either borrowed from a smaller person or had not kept up with his weight gain. When he bent over to examine the patient his shirt and trousers separated and the examiners thought he must have had a previous career as a plumber.
HINT
1.
Remember your bag lock combination number.
2.
Do not place your bag on a sink (or behind you on the floor).
3.
Make sure all your batteries are charged.
During practice sessions, it is always a good idea to place equipment in the same pockets each time. In the exam, you do not want to be fumbling at this crucial time – it will only create a poor impression. Consultants, other than cardiologists, carry their stethoscopes or put them in their coat pocket; rarely do they place them around their neck. This seems a sensible policy for aspiring consultants also. Candidates who do carry a briefcase into the test (and many neurologists carry one everywhere) can usually place it on the patient’s bedside table and leave it open so that its contents are easily accessible.
Some candidates take beta-blockers on the day of the test to remain calm. An interesting story from the
Lancet
highlights this very situation. A Scottish physician refers to a British censor who had the habit of counting the temporal pulse of candidates: if he found that the pulse rate was less than 60 beats/minute, he would take this fact into account when giving his mark (M G Bamber. Dope test for doctors.
Lancet
, 1980. ii:1308). We are unaware of a similar practice in Australasia. However, candidates intending to use these drugs should give themselves a dose during a practice session. One doctor who did not do this learnt to his horror during the actual examination that beta-blockers caused him severe bronchospasm (he failed).
Nervous individuals with a tendency to sweat can have problems. One candidate (now a professor), who was balding and wore glasses, found that during times of intense anxiety rivers of sweat would roll down from his forehead and fog up his glasses, washing them from his nose. His solution was antiperspirant (unscented, of course) applied generously to the forehead (he passed).
Dress is important. The medical establishment is well known for its conservatism, and the nonverbal messages that your appearance gives should not be forgotten when dressing. Traditionally, men and women wear a conservative suit and men a noncommittal tie. Almost all examiners wear suits and ties (or perhaps a bowtie). In fact, a suit (for both men and women) is a sort of uniform and by far the easiest thing to wear. The most important thing is not to wear something that will make you feel self-conscious and distract you from performing well in the exam itself.
Other important considerations for men are having short tidy hair, a neatly trimmed beard if you cannot bear to shave it off, and a neutral smell. Dress formally, with care to project an air of quiet efficiency. White coats are never worn. However, being well dressed is no guarantee of success. There is a story of two male candidates, wearing grey suits and with recently cut hair, who were viewing with satisfaction a third examinee whose long hair was tied neatly in a bun and who was dressed in a flowing Kaftan-like garment – they felt their own success assured with such competition. However, it turned out that they were unsuccessful and their colleague passed.
Preparation is the key to success. Like an Olympic athlete, obtain plenty of sleep in the week before the ordeal; take no alcohol or tranquillisers in the 48 hours before it; and do not study during the final 24 hours. Make sure that you eat something before the examination and avoid taking a long trip to the examination city on the morning of or the night before the test.
1
Diagnosis? See
p. 324
(
Fig 10.6
) for an answer.
2
The examiners are Simon O’Connor, holding the patella hammer, and Nick Talley observing intently.
CHAPTER 4
The long case
In what manner are the examiners elected? Are they elected by the profession or any part of the profession whose interests are equal to those of the whole and are they responsible to the profession at large for their conduct?
Neither the one nor the other.
Lancet 1824; i:20
When the examiners discuss a long case with a candidate they are expecting to find out how the candidate would manage the patient and his or her problems. They want to know whether the candidate has a practical grasp of what is required in consultant practice. Candidates are expected to have a mature and sensible approach to the patient and his or her problems. It may help to picture yourself as the physician taking over the care of a new patient. Practising long cases trains candidates to be better clinicians.
Careful allocation of time with the patient in the long case is vital. The exact proportions will depend on the case itself, but, as a rough guide, spend 25 minutes on the history-taking, 15 minutes on the examination and the rest of the time preparing discussion and reviewing vital facts with the patient. Remember though, that you can continue to ask the patient questions as these occur to you while you are examining. Nothing is more important than ensuring you leave enough time to put your thoughts in order.
Candidates favour many different systems for recording long-case details (as an aid to memory or
aide memoire
). There are two we recommend: one is to use a pad that can be held comfortably in the hand and the pages turned unobtrusively. Most candidates now use a large card folder, one side of which is used for the history and the other for the examination findings; a second card (if necessary) is used for relevant investigations, management and short lists of facts you may wish to mention. Obviously, numbering each side is important, so as not to mix up the order of presentation. These cards are usually provided to candidates who want them at the examination site. Mixing up the
cards can be a disaster. One candidate was sitting, preparing to enter the examination room, when the side door opened and a puff of wind blew the cards out of her hands. She was then ushered straight into the examination room with the cards in random order. She began the long case badly and failed.