i bc27f85be50b71b1 (9 page)
Read i bc27f85be50b71b1 Online
Authors: Unknown

Clinical Tip
•
When palpating HR, counting pulses for 1 5 seconds
and multiplying by 4 is sufficient with normal rates and
rhythms. [f rates are faster than 1 00 bpm or slower than
60 bpm, they should be palpated for 60 seconds. If the
rhythm is irregularly irregular (e.g., during atrial fibrillation) or regularly irregular (e.g., premature ventricular contractions [PVCs]), auscultation of heart sounds should
be performed to identify the apical HR for a full minute.








CARDIAC SYSTEM
t 7
Table 1-5. Pulse Amplitude Classification and Pulse Abnormalities
Pulse Amplitude Classification
Scale
Degree
Description
o
Absent pulse
No pulse-no circulation
1+
Diminished pulse
Reduced stroke volume and ejection fracrion, Increased vascular
resistance
2+
Normal pulse
Normal resting conditions, no
pathologies
3+
Moderately increased
Slightly increased stroke volume
and ejection fraction
4+
Markedly increased
Increased stroke volume and ejec
(boundlllg)'
tion fraction, can be diminished
with vasoconstriction
Pulse Abnormalities
Abnormality
Palpation
Description
Pulsus
Regular rhythm With
Indicates left ventricular failure
alternans
strong pulse waves
when present at normal heart
alternaring with
rares
weak pulse waves
Bigeminal
Every mher pulse is
Due ro preventricular contractions
pulses
weak and early
(bigeminy)
Pulsus
Reduction in strength
May be caused by chronic obstrucparadoxus
of the pulse with an
tive lung disease, pericarditis,
abnormal decline
pulmonary emboli, restrictive
in blood pressure
cardiomyopathy, and cardioduring inspiration
genic shock
·Corrigan's pulse IS a houndmg pulse viSible in the carotid artery rhat occurs with aorlIC rcgurgltallon.
Source: Data from SL Woods, ES SivaraJian-Froelichcr. S Underhill-Morzer (eds). Car·
dlac NurSing (4th cd). Philadelphia: Lippincott, 2000.
In these cases, palpation of pulse cannot substitute for
ECC analysis ro moniror the patient'S rhythm, but it may
alert the therapist to the onset of these abnormalities.
• Use caution in palpating pulses, as manual pressure on the
carotid sinus may cause reflexive drops in HR, BP, or both.

1 8 ACUTE CARE HANDBOOK FOR PHYSICAL TIIFRAI'ISTS
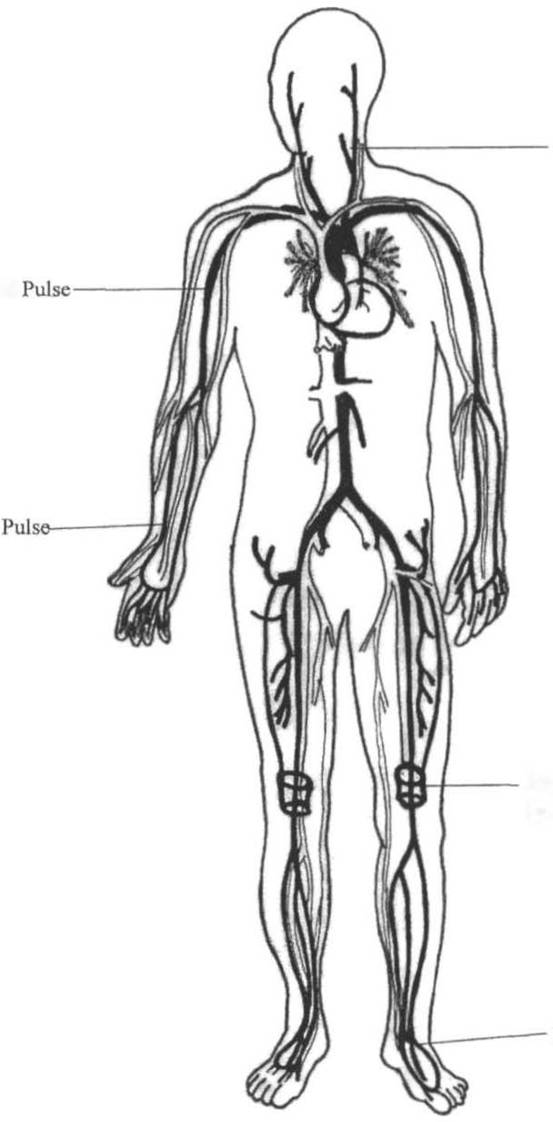
Carotid ulse
Brachial
Radial
Popliteal Pulse
(posterior knee)
Pedal Pulse
Figure 1 ·6. Arterial pulses. (Draw" by Barbara Cocauour, Ph.D., U"iversity
of Massachusetts, Lowell, Department of Physical Therapy.)