Ross & Wilson Anatomy and Physiology in Health and Illness (174 page)
Read Ross & Wilson Anatomy and Physiology in Health and Illness Online
Authors: Anne Waugh,Allison Grant
Tags: #Medical, #Nursing, #General, #Anatomy

B-lymphocytes are much less mobile than T-cells, and spend much of their time in lymphoid tissue, e.g. the spleen and lymph nodes. B-lymphocytes, unlike T-lymphocytes, recognise and bind antigen particles without having to be presented with them by an antigen-presenting cell. Once its antigen has been detected and bound, and with the help of an activated helper T-lymphocyte, the B-lymphocyte enlarges and begins to divide (clonal expansion,
Fig. 15.4
). It produces two functionally distinct types of cell, plasma cells and memory B-cells.
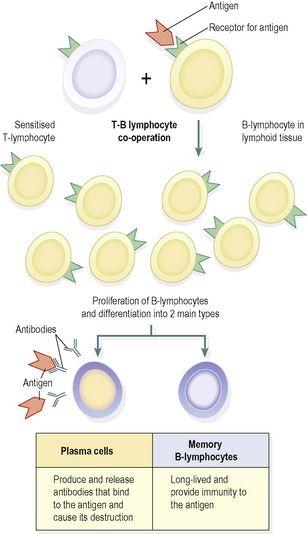
Figure 15.4
Clonal expansion of B-lymphocytes.
Plasma cells
These secrete massive quantities of antibodies (immunoglobulins) into the blood. Antibodies are carried throughout the tissues. Plasma cells live no longer than a day, and produce millions of molecules of only one type of antibody, which targets the specific antigen that originally bound to the B-lymphocyte. Antibodies:
•
bind to antigens, labelling them as targets for other defence cells such as cytotoxic T-lymphocytes and macrophages
•
bind to bacterial toxins, neutralising them
•
activate complement (
p. 367
).
There are five main types of antibody, summarised in
Table 15.2
.
Table 15.2
The five types of antibody
| Type of antibody | Function |
|---|---|
| IgA | Found in body secretions like breast milk and saliva, and prevent antigens crossing epithelial membranes and invading deeper tissues |
| IgD | This is made by B-cells and displayed on their surfaces. Antigens bind here to activate B-cells |
| IgE | Found on cell membranes of, e.g., basophils and mast cells, and if it binds its antigen, activates the inflammatory response. This antibody is often found in excess in allergy |
| IgG | This is the largest and most common antibody type. It attacks many different pathogens, and crosses the placenta to protect the fetus |
| IgM | Produced in large quantities in the primary response and is a potent activator of complement |
Memory B-cells
Like memory T-cells, these cells remain in the body long after the initial episode has been dealt with, and rapidly respond to another encounter with the same antigen by stimulating the production of antibody-secreting plasma cells.
The interdependence of the two parts of the immune system is summarised in
Figure 15.5
.
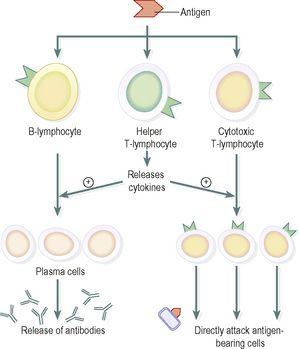
Figure 15.5
Interdependence of the T- and B-lymphocyte systems in the immune response.
The fact that the body does not normally develop immunity to its own cells is due to the fine balance that exists between the immune reaction and its suppression.
Autoimmune diseases
are due to the disturbance of this balance.
Acquired immunity
The immune response to an antigen following the first exposure (primary immunisation) is called the
primary response
. Second and subsequent exposures give rise to a
secondary response
(
Fig. 15.6
).
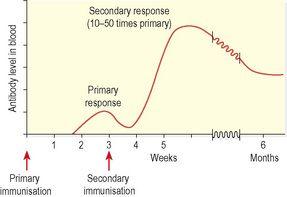
Figure 15.6
The antibody responses to antigen exposure.
The primary response
Exposure of the immune system to an antigen for the first time leads to a slow and delayed rise in antibody levels, peaking 1–2 weeks after infection. This delayed response reflects the time required to activate the T-lymphocyte system, which then stimulates B-lymphocyte division. Antibody levels start to fall once the infection is cleared, but if the immune system has responded well, it will have generated a population of long-lived memory B-cells, making the individual immune to future infection.
The secondary response
On subsequent exposures to the same antigen, the immune response is much faster and significantly more powerful, because the memory B-lymphocytes generated after the first infection rapidly divide and antibody production begins almost immediately.
Immunity may be acquired
naturally
or
artificially
and both forms may be active or passive (
Fig. 15.7
). Active immunity means that the individual has responded to an antigen and produced his own antibodies, lymphocytes are activated and the memory cells formed provide long-lasting resistance. In passive immunity the individual is given antibodies produced by someone else. The antibodies eventually break down, so passive immunity is relatively brief.
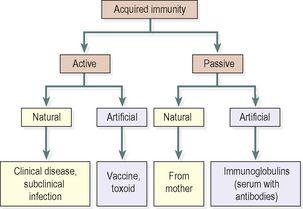
Figure 15.7
Summary of the types of acquired immunity.
Active naturally acquired immunity
The body may be stimulated to produce its own antibodies by:
•
Having the disease
. During the course of the illness, B-lymphocytes develop into plasma cells that produce antibodies in sufficient quantities to overcome the infection. After recovery, the memory B-cells produced confer immunity to future infection by the same antigen.
•
Having a subclinical infection
. Sometimes the infection is not sufficiently severe to cause clinical disease but stimulates sufficient memory B-cells to establish immunity. In other cases, subclinical infection may be too mild to stimulate an adequate response for immunity to develop.
Active artificially acquired immunity
This type of immunity develops in response to the administration of dead or live artificially weakened pathogens (
vaccines
) or deactivated toxins (
toxoids
). The vaccines and toxoids retain the antigenic properties that stimulate the development of immunity but they cannot cause the disease. Many infectious diseases can be prevented by artificial immunisation. Examples are shown in
Box 15.1
.

Box 15.1
Diseases preventable by vaccination
•
Anthrax
•
Cholera
•
Diphtheria
•
Hepatitis B
•
Measles
•
Mumps
•
Poliomyelitis
•
Rubella
•
Smallpox
•
Tetanus
•
Tuberculosis
•
Typhoid
•
Whooping cough
Active immunisation against some infectious disorders gives lifelong immunity, e.g. diphtheria, whooping cough or mumps. In other infections the immunity may last for a number of years or for only a few weeks before revaccination is necessary. Apparent loss of immunity may be due to infection with a different strain of the same pathogen, which has different antigenic properties but causes the same clinical illness, e.g. viruses that cause the common cold and influenza. In older or poorly nourished individuals, lymphocyte production, especially B-lymphocytes, is reduced and the primary and secondary response may be inadequate.