Ross & Wilson Anatomy and Physiology in Health and Illness (175 page)
Read Ross & Wilson Anatomy and Physiology in Health and Illness Online
Authors: Anne Waugh,Allison Grant
Tags: #Medical, #Nursing, #General, #Anatomy

Passive naturally acquired immunity
This type of immunity is acquired before birth by the passage of maternal antibodies across the placenta to the fetus, and to the baby in breast milk. The variety of different antibodies provided depends on the mother’s active immunity. The baby’s lymphocytes are not stimulated and the immunity is short lived.
Passive artificially acquired immunity
In this type, ready-made antibodies, in human or animal serum, are injected into the recipient. The source of the antibodies may be an individual who has recovered from the infection, or animals, commonly horses, that have been artificially actively immunised. Specific immunoglobulins (antiserum) may be administered
prophylactically
to prevent the development of disease in people who have been exposed to the infection, or
therapeutically
after the disease has developed.
Abnormal immune function

Learning outcomes
After studying this section, you should be able to:
describe, with examples, the four types of allergic response
Hypersensitivity (allergy)
Allergy is powerful immune response to an antigen (allergen). The allergen itself is usually harmless (e.g. house dust, animal dander, grass pollen). It is therefore usually the immune response that causes the damage to the body, not the allergen itself. Upon initial exposure to the allergen the individual becomes sensitised to it, and on second and subsequent exposures the immune system mounts a response entirely out of proportion to the perceived threat. It should be noted that these responses are exaggerated versions of normal immune function (secondary response,
Fig. 15.6
). Sometimes symptoms are mild, if annoying, e.g. the running nose and streaming eyes of hay fever. Occasionally the reaction can be extreme, overwhelming body systems and causing death, e.g. anaphylactic shock, see below.
There are four mechanisms of hypersensitivity, which are classified according to what parts of the immune system are involved. They are summarised in
Figure 15.8
.
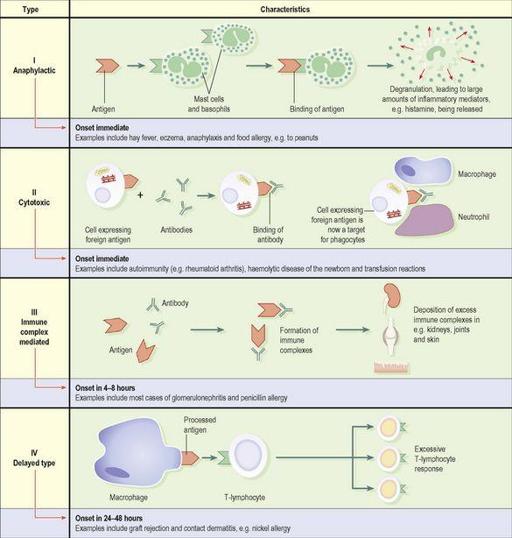
Figure 15.8
The four types of hypersensitivity.
Type I, anaphylactic hypersensitivity
This occurs in individuals who have inherited very high levels of immunoglobulin E (IgE). When exposed to an allergen, e.g. house dust, these high levels of antibody activate mast cells and basophils (
p. 62
), which release their granular contents. The most important substance released is histamine, which constricts some smooth muscle, e.g. airway smooth muscle, causes vasodilation and increases vascular permeability (leading to exudation of fluid and proteins into the tissues). Examples of type I reactions include the serious situation of anaphylaxis. There is profound bronchoconstriction and shock (
p. 111
) due to extensive vasodilation. The condition can lead to death.
Type II, cytotoxic hypersensitivity
When an antibody reacts with an antigen on a cell surface, that cell is marked for destruction by a number of mechanisms, e.g. phagocytosis, or destruction by lytic enzymes. This is the usual procedure in the elimination of, for example, bacteria, but if the antibodies are directed against self-antigens the result is destruction of the body’s own tissues (autoimmune disease). Type II mechanisms cause other conditions, e.g. haemolytic disease of the newborn (
p. 68
) and transfusion reactions (
p. 69
).
Type III, immune-complex-mediated hypersensitivity
Antibody–antigen complexes (immune complexes) are usually cleared efficiently from the blood by phagocytosis. If they are not, for example when there is phagocyte failure or an excessive production of immune complexes (e.g. in chronic infections), they can be deposited in tissues, e.g. kidneys, skin, joints and the eye, where they set up an inflammatory reaction. The kidney is a common site of deposition because it receives a large proportion of the cardiac output and filters the blood. Immune complexes collecting here lodge in and block the glomeruli (
p. 331
), impairing kidney function (glomerulonephritis). Sensitivity to penicillin is also a type III reaction; antibodies bind to penicillin (the antigen), and the symptoms are the result of deposition of immune complexes in tissues – rashes, joint pains and sometimes haematuria.
Type IV, delayed type hypersensitivity
Unlike types I–III, type IV hypersensitivity does not involve antibodies, but is an overreaction of T-lymphocytes to an antigen. When an antigen is detected by memory T-lymphocytes, it provokes clonal expansion of the T-lymphocyte (
Fig. 15.3
), and large numbers of cytotoxic T-lymphocytes are released to eliminate the antigen. Usually this system is controlled and the T-lymphocyte response is appropriate. If not, the actively aggressive cytotoxic T-lymphocytes damage normal tissues.
An example of this is contact dermatitis (
p. 362
). Graft rejection is also caused by T-lymphocytes; an incompatible skin graft, for instance, will become necrotic and slough off in the days following application of the graft.
Autoimmune diseases
Normally, an immune response is mounted only against foreign (non-self) antigens, but occasionally the body fails to recognise its own tissues and attacks itself. The resulting autoimmune disorders, examples of type II hypersensitivity, include a number of relatively common conditions.
Rheumatoid arthritis (
p. 422
)
The body produces antibodies to the synovial membranes (
p. 402
). In most sufferers, the antibody can be detected in the blood. Called
rheumatoid factor
, it binds to the synovial membrane, leading to chronically inflamed joints that are stiff, painful and swollen.