Pocket Medicine: The Massachusetts General Hospital Handbook of Internal Medicine (28 page)
Read Pocket Medicine: The Massachusetts General Hospital Handbook of Internal Medicine Online
Authors: Marc Sabatine
Tags: #Medical, #Internal Medicine

BOOK: Pocket Medicine: The Massachusetts General Hospital Handbook of Internal Medicine
10.53Mb size Format: txt, pdf, ePub
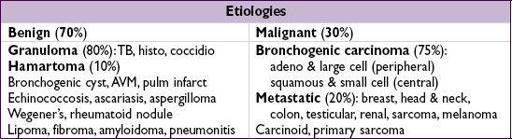
Initial evaluation
•
History
: h/o cancer, smoking, age (<30 y = 2% malignant, +15% each decade >30) •
CT
: size/shape, Ca
2+
, LAN, effusions, bony destruction,
compare w/ old studies
Ø Ca → ↑ likelihood malignant; laminated → granuloma; “popcorn” → hamartoma
• High-risk features for malignancy: ≥2.3 cm diameter, spiculated, >60 yo, >1 ppd current smoker, no prior smoking cessation (
NEJM
2003;348:2535)
Diagnostic studies
•
PET
: detects metab. activity of tumors, 97% Se & 78% Sp for malig. (esp. if >8 mm) also useful for surgical staging b/c may detect unsuspected mets (
JAMA
2001;285:914) useful in deciding which lesions to bx vs. follow w/ serial CT (
J Thor Oncol
2006;1:71) •
Transthoracic needle biopsy (TTNB)
: if tech. feasible, 97% will obtain definitive tissue dx (
AJR
2005;185:1294); if noninformative or malignant → resect •
Video-assisted thoracoscopic surgery
(VATS): for percutaneously inaccessible lesions; highly sensitive and allows resection; has replaced thoracotomy • Transbronchial bx (TBB): most lesions too small to reliably sample w/o endobronchial U/S (
Chest
2003;123:604); bronch w/ brushings low-yield unless invading bronchus; navigational bronchoscopy w/ 70% yield, ↑ sens w/ larger nodules (
Chest
2012;142:385) • PPD, fungal serologies, ANCA
Management
(for solid SPN
>8 mm; if ≤8 mm, serial CT) (
Chest
2013;143:840)
•
Low risk
(<5%, see ref): serial CT (freq depending on risk); shared decision w/ Pt re: bx •
Intermediate risk
(5–60%): PET, if→ follow low-risk protocol; if
→ high-risk protocol •
High risk
(and surgical candidate): TBB, TTNB, or VATS → lobectomy if malignant •
Ground-glass nodules:
longer f/u b/c even if malignant can be slow-growing and PET
OBSTRUCTIVE SLEEP APNEA (OSA)
Definition and pathophysiology
• Repetitive pharyngeal collapse during sleep causing apnea (≥10 s) or hypopnea (airflow reduction) ± desaturation, arousals from sleep → daytime sleepiness • Apnea-hypopnea index = avg # apneas and hypopneas per hr of sleep • Sleep-induced loss of activity of pharyngeal dilator muscles → pharyngeal collapse → arousal → activation of sympathetic nervous system; phenotypes vary across OSA Pts • Apnea → negative intrathoracic pressure → ↑ preload, ↑ afterload → HTN, CV sequelae • Risk factors: obesity (present in 70%), male, age, alcohol, smoking, black race
Clinical manifestations
(
Lancet
2002;360:237;
Lancet Resp Med
2013;1:61)
• Snoring, witnessed apneas/gasping, daytime sleepiness •
Cardiovascular
: HTN (
JAMA
2012;307:2169); a/w ↑ risk of stroke and death (
NEJM
2005;353:2034) & possibly CAD & endothelial dysfxn (
AJRCCM
2001;163:19;
Circ
2008;117:2270) •
Neurocognitive
: ↓ cognitive performance, ↓ QoL, ↑ motor vehicle and work accidents (
NEJM
1999;340:847;
AJRCCM
2001;164:2031)
Diagnosis and treatment
•
Polysomnography
(sleep study); can do home-testing. If
•
CPAP
: ↓↓ apnea/hypopnea, ↓ BP (
Lancet
2002;359:204), ↓ sleepiness, ↑ performance (
AJRCCM
2012;186:677), ↑ EF in Pts with CHF (
NEJM
2003;348:1233), ↓ metab syndrome (
NEJM
2011;365:2277), ↓ mortality after stroke (
AJRCCM
2009;180:36) • Oral appliances can prevent retroglossal collapse. Offer if refusing CPAP.
• Avoid alcohol and sedatives • Surgery (eg, uvulopalatopharyngoplasty, UPPP) of limited benefit (
Chest
1997;111:265)
INTERSTITIAL LUNG DISEASE
WORKUP OF ILD
Rule out mimickers of ILD
•
Congestive heart failure
(✓ BNP, trial of diuresis) •
Infection
: viral, atypical bacterial, fungal, mycobacterial, parasitic •
Malignancy
: lymphangitic carcinomatosis, bronchoalveolar, leukemia, lymphoma
History and physical exam
• Occupational, travel, exposure (including tobacco), meds, FHx, precipitating event • Tempo (acute → infxn, CHF, hypersens pneumonitis, eos PNA, AIP, COP, drug-induced) • Extrapulmonary s/s (skin Ds, arthralgias/arthritis, clubbing, neuropathies, etc.)
Diagnostic studies
(see Appendix & Radiology inserts)
• CXR and
high-resolution chest CT
: reticular, nodular or ground glass pattern upper → coal, silicon, hypersens, sarcoid, TB, RA; lower → IPF, asbestos, scleroderma adenopathy → sarcoidosis, berylliosis, silicosis, malignancy, fungal infections pleural disease → collagen-vascular diseases, asbestosis, infections, XRT
• PFTs: ↓ D
L
CO (
early sign
), restrictive pattern (↓ volumes), ↓ P
a
O
2
(esp. w/ exercise); if also obstructive, consider sarcoid, LAM, silicosis • Serologies: ✓ ACE, ANA, RF, ANCA, anti-GBM, HIV
• Bronchoalveolar lavage: dx infxn, hemorrhage, eosinophilic syndromes, PAP
• Biopsy (transbronch, CT-guided, VATS, open) if no clear precipitant and w/u unrevealing
ETIOLOGIES OF ILD
Sarcoidosis
(
NEJM
2007;357:2153;
JAMA
2011;305:391)
• Prevalence: African Americans, northern Europeans and females; onset in 3rd–4th decade • Pathophysiology: depression of cellular immune system peripherally, activation centrally
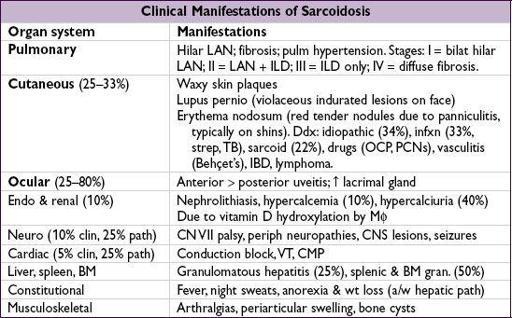
•
Löfgren’s syndrome
: erythema nodosum + hilar adenopathy + arthritis (good prognosis) • Diagnostic studies:
LN bx
→
noncaseating granulomas
+ multinucleated giant cells
18
FDG PET can be used to identify extent and potentially targets for dx bx ↑
ACE
(Se 60%, 90% w/ active dis., Sp 80%, false
steroids
(eg, prednisone 20–40 mg/d) if sx or extrathoracic organ dysfxn (improves sx, but doesn’t Δ long-term course); hydroxychloroquine for extensive skin disease; anti-TNF, MTX, AZA, mycophenolate or cyclophosphamide for chronic/refractory disease • Prognosis: ~
2
/
3
spontaneously remit w/in 10 y (60–80% of stage I, 50–60% stage II, 30% stage III), w/ relapses uncommon; ~
1
/
3
have progressive disease
Iatrogenic
Other books
Fated by Courtney Cole
Outside the Box by H. M. Montes
How to Lose 10 Pounds in a Week by Jenny Allan
A Warrior for Christmas by Beth Trissel
Wife in Public by Emma Darcy
Magical Passes by Carlos Castaneda
The Mark-2 Wife by William Trevor
Dave Cameron and the Extraterrestrial by V Bertolaccini
The Truth About Butterflies: A Memoir by Nancy Stephan