Pocket Medicine: The Massachusetts General Hospital Handbook of Internal Medicine (53 page)
Read Pocket Medicine: The Massachusetts General Hospital Handbook of Internal Medicine Online
Authors: Marc Sabatine
Tags: #Medical, #Internal Medicine

BOOK: Pocket Medicine: The Massachusetts General Hospital Handbook of Internal Medicine
2Mb size Format: txt, pdf, ePub
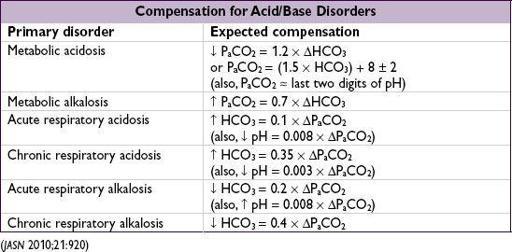
Mixed disorders
(more than one primary disorder at the same time)
• If compensation less or greater than predicted, may be 2 disorders:
P
a
CO
2
too low → concomitant 1° resp. alk.
P
a
CO
2
too high → concomitant 1° resp. acid.
HCO
3
too low → concomitant 1° met. acid.
HCO
3
too high → concomitant 1° met. alk.
• Normal pH
but
…
↑ P
a
CO
2
+ ↑ HCO
3
→ resp. acid. + met. alk.
↓ P
a
CO
2
+ ↓ HCO
3
→ resp. alk. + met. acid.
normal P
a
CO
2
& HCO
3
,
but
↑ AG → AG met. acid. + met. alk.
normal P
a
CO
2
, HCO
3
, & AG → no disturbance
or
non-AG met. acid. + met. alk.
•
Cannot
have resp. acid. (hypoventilation) and resp. alk. (hyperventilation) simultaneously
Figure 4-1 Acid-base nomogram
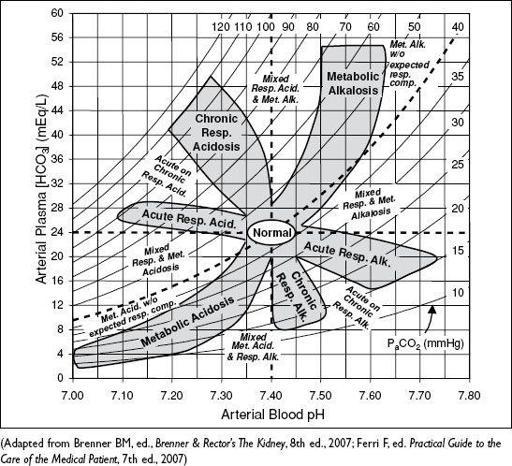
•
ABG vs. VBG
: concordant for pH (~0.04), HCO
3
(~2 mEq) but
not
P
a
CO
2
(~8±17 mmHg) VBG can be used to
screen
for hypercarbia w/ P
a
CO
2
cutoff ≥45 mmHg (100% Se),
but
does not accurately assess
degree
of hypercarbia (
Am J Emerg Med
2012;30:896)
METABOLIC ACIDOSIS
Initial workup
(
Nat Rev Nephol
2010;6:274)
• ✓
anion gap
(AG) = Na+ – (Cl
-
+ HCO
3
-
) = unmeasured anions - unmeasured cations
if ↑ glc, use measured
not
corrected Na
expected AG is [albumin] × 2.5 (ie, 10 if albumin is 4 g/dL, 7.5 if albumin is 3 g/dL)
↑ AG → ↑ unmeasured anions such as organic acids, phosphates, sulfates
↓ AG → ↓ alb or ↑ unmeasured cations (Ca, Mg, K, Li, bromine, immunoglobulin)
• If ↑ AG, ✓
delta-delta
(ΔΔ = DAG/DHCO
3
) to assess if there is an additional metabolic acid-base disturbance; DAG = (calculated AG – expected AG), DHCO
3
= (24 – HCO
3
)
ΔΔ = 1–2 → pure AG metabolic acidosis
ΔΔ < 1 → AG metabolic acidosis
and
simultaneous non-AG acidosis
ΔΔ > 2 → AG metabolic acidosis
and
simultaneous metabolic alkalosis
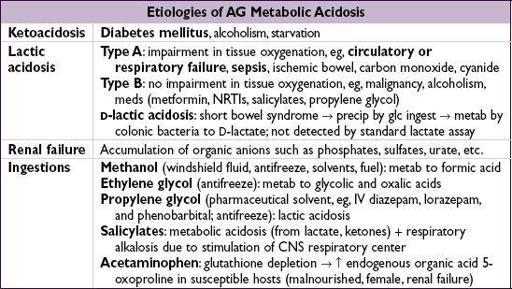
Workup for AG metabolic acidosis
• ✓ for
ketonuria
(dipstick acetoacetate) or plasma b-hydroxybutyrate (bOHB) nb, urine acetoacetate often not present in early ketoacidosis due to shunting to bOHB; ∴ acetoacetate may later turn, but does not signify worsening disease
• Ifketones, ✓
renal function
,
lactate
,
toxin screen
, and
osmolal gap
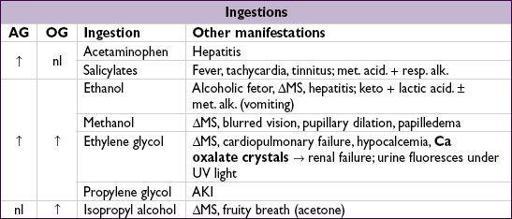
•
Osmolal gap
(OG) = measured osmoles – calculated osmoles
calculated osmoles = (2 × Na) + (glucose
18) + (BUN
2.8) (can + [EtOH/4.6] if have EtOH level and want to test if other ingestions)
OG >10 → suggests ingestion (see below)
for methanol/ethylene glycol: early on, OG precedes AG; later OG may be nl with
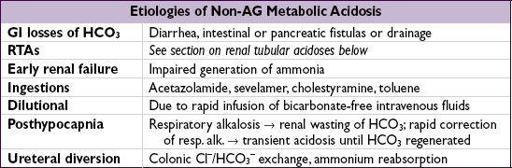
Workup for non-AG metabolic acidosis
(
CJASN
2012;7:671)
• Evaluate history for causes (see above)
• ✓
urine anion gap
(UAG) = (U
Na
+ U
K
) – U
Cl
UAG = unmeasured anions – unmeasured cations; as NH
4
+ is primary unmeasured cation, UAG is indirect assay for renal NH
4
+ excretion (
NEJM
1988;318:594)
•
4
+ excretion → appropriate renal response to acidemia Ddx: GI causes, proximal RTA, ingestions or dilutional
Other books
Just Your Average Princess by Kristina Springer
The Call by Michael Grant
Let's Talk of Murder by Joan Smith
Love Found Me (A City Love Novel, Book 1) by Amari, Nina
Devoured by Emily Snow
Season of Secrets by Marta Perry
Operation Honshu Wolf by Addison Gunn
My First Murder by Leena Lehtolainen
The Night of the Burning by Linda Press Wulf