Pocket Medicine: The Massachusetts General Hospital Handbook of Internal Medicine (89 page)
Read Pocket Medicine: The Massachusetts General Hospital Handbook of Internal Medicine Online
Authors: Marc Sabatine
Tags: #Medical, #Internal Medicine

BOOK: Pocket Medicine: The Massachusetts General Hospital Handbook of Internal Medicine
8.45Mb size Format: txt, pdf, ePub
Microbiology & natural history
• Transmission of
Mycobacterium tuberculosis
via small-particle aerosols (droplet nuclei) • 90% of infected normal hosts will never develop clinically evident disease • Localized disease: healing & calcification
or
progressive 1° TB (at site of infection) • Hematogenous spread: latent infection ± reactivation TB
or
progressive dissem. TB
Screening for prior infection
•
Whom to screen
: high-prevalence and high-risk populations (HIVPts should have PPD testing as part of initial evaluation and annually thereafter) •
How to screen
: Mantoux tuberculin test (ie, purified protein derivative or PPD) inject 5-TU (0.1 mL) intermed. strength PPD
intradermally
→ wheal; examine 48–72 h •
How to interpret PPD
: determine max. diameter of induration by palpation
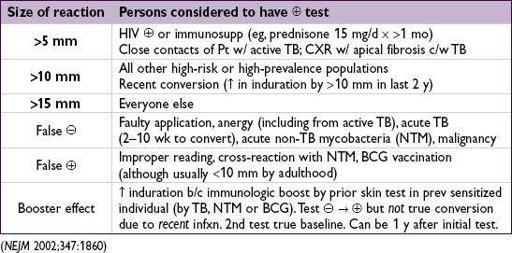
•
IFN-
γ
release assays (IGRA)
: (Ag-stimulated IFN-g release from Pt’s T-cells): can be used for screening where you would use PPD (
MMWR
2010;59:1); ↑ Sp, esp. in BCG Rx’d Pts (
Annals
2008;149:177). Does not distinguish active vs. latent, or recent vs. remote infxn. Relies on host immune fxn; Se limited in immunosupp. Lack of gold standard for latent TB infxn compromises Se/Sp estimates (
J Clin Epi
2010;63:257;
CID
2011;52:1031).
Clinical manifestations
•
Primary TB pneumonia
: middle or lower lobe
consolidation
, ± effusion, ± cavitation •
TB pleurisy
: can occur w/ primary or reactivation. Due to breakdown of granuloma w/ spilling of contents into pleural cavity and local inflammation.
Pulmonary effusion
± pericardial and peritoneal effusions (tuberculous polyserositis).
•
Reactivation TB pulmonary disease
: apical infiltrate ± volume loss ± cavitation •
Miliary TB
: acute or insidious; due to widespread hematogenous dissemination; usually in immunosupp, DM, EtOH, elderly or malnourished.
Constitutional sx
(fever, night sweats, weight loss) usually prominent. Pulm disease w/ small millet seed-like lesions (2– 4 mm) on CXR or chest CT (latter more Se) present in 60–80% of those w/ miliary TB.
•
Extrapulmonary TB
: lymphadenitis, pericarditis, peritonitis, meningitis, nephritis ± sterile pyuria, osteomyelitis (vertebral = Pott’s disease), hepatitis, splenitis, cutaneous, arthritis •
TB and HIV
: HIV
Diagnostic studies for active TB
(
high index of suspicion is key!
)
•
AFB smear
(rapid dx) and
culture
(↑ Se & allows sensitivity testing) of sputum, BAL, pleura, etc.;
avoid FQ
if considering TB (can compromise dx yield) • PCR: 94–97% Se c/w smear; 40–77% Se c/w culture (
JAMA
2009;301:1014) • CXR: classically fibrocavitary apical disease in reactivation vs. middle & lower lobe consolidation in 1° TB, but distinction imperfect. HIV
JAMA
2005;293:2740).
• Adenosine deaminase testing: useful in extrapulmonary sites, best validated for ascites
Preventive therapy
(
Annals
2009;150:ITC6-1;
NEJM
2010;362:707)
• Prophylaxis reduces incidence of subsequent disease by 65–75%
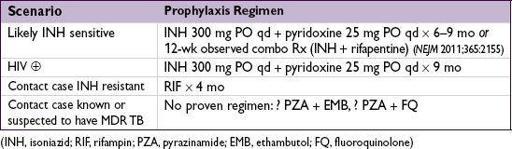
• Treat Pts who are
R/o active disease
in any Pt w/ suggestive s/s before starting INH. If HIV
• ✓ LFTs monthly (risk ↑ w/ age;
Chest
2005;
1
28:
11
6
): if 5× ULN
or
sx → stop TB meds & reeval
Treatment of active tuberculosis
(
Annals
2009;150:ITC6-1;
NEJM
2013;368:745)
• Isolate Pt per infection control if hospitalized, modified isolation per Dept of Health if outPt • Use multiple drugs (see below) to which organism susceptible; consult ID before empiric Rx if possible MDR-TB (suspect if prior TB Rx, from or travel to area w/ ↑ rates of MDR, exposure to person w/ likely MDR-TB, poor Rx adherence) or if INH resistance in community ≥4% (includes most of U.S.), extrapulm. TB or HIV
NEJM
2008;359:636) • Screen for HIV in Pts starting TB Rx; if HIVfor TB
Other books
Beyond a Misty Shore by Lyn Andrews
Fated Folly by Elizabeth Bailey
Losing Control by Jarman, Jessica
The Valley of the Shadow by Carola Dunn
The Opportunist by Tarryn Fisher
Mortal Fear by Mortal Fear
Golden Boy by Martin Booth
Michael Tolliver Lives by Armistead Maupin
demon slayer 05.5 - the tenth dark lord a leaping by fox, angie
Her Two Billionaires and a Baby by Julia Kent